|
|
|
|
|
|
Amebiasis
-
-
Causative agent of amebiasis: protozoan parasite Entamoeba histolytica
-
Two distinct (morphologically identical species) in the Entamoeba complex
-
E. dispar-resides in the colon; as a stable commensal
-
E. histolytica (10% of the complex)-shows virulence (varying degrees)
-
Severe intestinal infection (dysentery)
-
Mild/moderate symptomatic intestinal infection
-
Asymptomatic intestinal infection
-
Ameboma
-
Liver abscess or other type of extraintestinal infection
-
-
-
-
-
Suggestive:
-
Primary: Travelers/immigrants (from E histolytica-endemic regions)-presenting with intestinal symptoms which a range from mild complaints to acute fulminant colitis.
-
-
Definitive:
-
Cysts or trophozoites in stool or rectal biopsy or trophozoites in other organs, e.g. the liver
-
95% sensitivity of serology in patients with extraintestinal amebiasis
-
Serology assay much less sensitive in patient with intestinal amebiasis
-
Serologic response: may remain positive for years.
-
-
-
-
Clinical Manifestations-Subjective
-
Intestinal Amebiasis:
-
90% of infected individuals: asymptomatic (most do not develop illness; infection clears within weeks or months spontaneously)
-
Symptomatic patient-noninvasive disease {only cysts}:
-
Abdominal pain
-
Increased bowel movement frequency
-
Increasing bowel movement frequency may be intermittent and may alternate with constipation
-
-
Symptomatic patients-invasive disease {only trophozoites seen}
-
Symptoms gradual, nonspecific
-
Abdominal pain
-
Watery diarrhea
-
Blood + mucus in stool {amebic dysentery}
-
Other symptoms relatively mild (appetite often retained) -- generally in contrast to invasive bacterial diarrheas.
-
With colitis present-segmental ulceration may occur:
-
Coalescing of segmental ulcers can become superinfected (bacterial) and may lead to toxic megacolon (unlikely)
-
Ulcerations may perforate, causing peritonitis-alternatively ulcerations may become fibrotic ultimately forming an ameboma.
-
-
-
-
Extraintestinal Amebiasis (Amebic Liver Abscess)
-
Occurs as a result of previous intestinal infection and may occur concurrently with colitis (frequency: 15%)
-
Typically:
-
No history of intestinal amebiasis
-
Stool examination -- negative
-
-
Symptoms/characteristics of liver abscess
-
Acute onset
-
Abdominal dull pain localized to right upper quadrant, epigastrum
-
Dull right shoulder pain-
-
If abscess is in the left liver lobe-pain can radiate to the left shoulder
-
-
Patients are likely (frequency: 90%) to have fever, malaise and become anorexic.
-
-
-
-
Clinical Manifestations: Objective
-
Intestinal Amebiasis
-
Physical Exam:
-
Relatively non-ill patient-nonspecific findings
-
Possible lower quadrant pain to palpation
-
Some hepatic tenderness
-
Hepatomegaly (abscess not required)
-
-
More seriously ill patient:
-
"Toxic" appearance with dehydration
-
Abdominal pain (diffuse)
-
Possible palpable mass (ameboma)
-
Possible colonic distention {toxic megacolon}
-
-
-
Laboratory: may be normal; most patients-heme-positive stool
-
-
Extraintestinal Amebiasis (amebic liver abscess)
-
Physical Exam:
-
Most Important Sign: Liver enlargement + pain on palpation (point tenderness, a frequent finding)
-
If abscess located high under diaphragm:
-
Intercostal tenderness
-
Dullness to percussion over right lower chest
-
Decreased breath sounds
-
-
-
Laboratory:
-
> 50% anemia, leukocytosis {left shift}
-
High fevers: common
-
Jaundice: rare
-
Eosinophilia: absent
-
Often minimal abnormalities in liver tests
-
-
-
Differential Diagnosis (Primary Reference: Morgan, Juliette and del Rio, Carlos, Amebiasis in Medicine for the Practicing Physician (Hurst, J. W., ed) Appleton-Lange, 1996, pp. 457-459.)
-
Overview:-intestinal amebiasis
-
Consider other infectious/noninfectious diarrhea causes and gastrointestinal disease in immigrants/travelers from endemic areas
-
-
Intestinal Amebiasis:
-
Diagnostic key: stool examination {routine lab tests: not useful}
-
Difficulties in performing correct stool examinations
-
Common false-positives and false-negatives
-
False Negatives caused by:
-
Antimicrobial agents
-
Soap/tap water enemas (lyse trophozoites)
-
Particular to matter (barium or bismuth)-obscures organisms
-
-
False Positives caused by:
-
Leukocytes misread as amebas
-
Other amebas confused with E. histolytica
-
-
-
Should take multiple stool samples (one "negative" stool result is not sufficient to rule out intestinal amebiasis)
-
Samples must be properly maintained if not analyzed immediately
-
-
Presence of many fecal leukocytes suggests some other diagnosis since E. histolytica causes lysis of neutrophils
-
Amebiasis differentiation from bacterial diarrheal disease, e.g.shigellosis
-
-
Indirect hemagglutination test: 70% sensitivity in patients with active intestinal disease-- only 10% sensitivity in asymptomatic cyst carrier
-
-
Overview: Extraintestinal Amebiasis:-
-
Differential includes:
-
Pyrogenic abscess
-
Usually multiple abscesses
-
Associated with biliary tract disease or other intraabdominal disease
-
-
Metastatic/primary tumor (includes hemangioma)
-
-
Typical amebic abscess:
-
Single
-
Right lobe
-
-
-
Extraintestinal Amebiasis:
-
Serology helpful if patient not from an endemic area
-
Diagnosis made based on:
-
Epidemiological information
-
Radiographic findings
-
Ultrasonography-most cost-effective; slightly less sensitive than other techniques
-
MRI
-
CT
-
Radioisotope liver scans
-
-
Positive serology
-
Most sensitive: indirect hemagglutination (95 percent sensitivity in extraintestinal disease) -- does not differentiate present from past infection
-
-
-
-
-
-
"A wide spectrum, from asymptomatic carriers ("luminal amebiasis"), to invasive intestinal amebiasis (dysentery, colitis, appendicitis, toxic megacolon, amebomas), to invasive extraintestinal amebiasis (liver abcess, peritonitis, pleuropulmonary abcess, cutaneous and genital amebic lesions)."-CDC
-
-
Life-cycle/Laboratory/Microscopy
-
Life Cycle Entamoeba histolytica
-
-
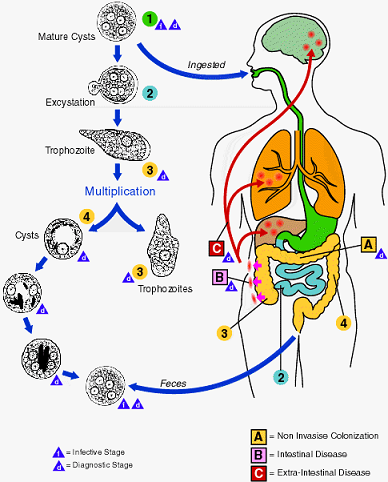
"Infection by Entamoeba histolytica occurs by ingestion of mature cysts 1 in fecally contaminated food, water, or hands.
-
Excystation 2 occurs in the small intestine and trophozoites 3 are released, which migrate to the large intestine. The trophozoites multiply by binary fission and produce cysts 4 , which are passed in the feces.
-
Because of the protection conferred by their walls, the cysts can survive days to weeks in the external environment and are responsible for transmission.
-
(Trophozoites can also be passed in diarrheal stools, but are rapidly destroyed once outside the body, and if ingested would not survive exposure to the gastric environment.)
-
In many cases, the trophozoites remain confined to the intestinal lumen ( A: non-invasive infection) of individuals who are thus asymptomatic carriers and cysts passers. In some patients the trophozoites invade the intestinal mucosa ( B: intestinal disease), or, through the bloodstream, extraintestinal sites such as the liver, brain, and lungs ( C: extra-intestinal disease), with resultant pathologic manifestations. It has been established that the invasive and noninvasive forms represent separate species, respectively E. histolytica and E. disparindistinguishable.
-
-
Transmission can , which are morphologically also occur through fecal exposure during sexual contact (in which case not only cysts, but also trophozoites could prove infective)."
-
Courtesy of the Division of Parasitic Diseases at the National Center for Infectious Diseases, Centers for Disease Control and Prevension (public domain)
-
-
-
Laboratory Diagnosis
-
Entamoeba histolytica must be differentiated from other intestinal protozoa such as the nonpathogenic amebas E. coli, E. hartmanni, E. polecki, E. gingivalis, Endolimax nana, and Iodamoeba bütschlii, and from the possibly pathogenic Dientamoeba fragilis (which is not an ameba but a flagellate).
-
Differentiation is possible (but not always easy) based on morphologic characteristics of the cysts and trophozoites. The nonpathogenic Entamoeba dispar, however, is morphologically identical to E. histolytica, and differentiation must be based on isoenzymatic, immunologic, or molecular analysis.
-
Microscopic identification of cysts and trophozoites in the stool is the common method for diagnosing E. histolytica. This can be accomplished using:
-
Fresh stool: wet mounts and permanently stained preparations (e.g. trichrome). Concentrates from fresh stool:
-
wet mounts, with or without iodine stain, and permanently stained preparations (e.g. trichrome). Concentration procedures, however, are not useful for demonstrating trophozoites.
-
-
In addition, E. histolytica trophozoites can also be identified in aspirates or biopsy samples obtained during colonoscopy or surgery.
-
-
Microscopy 2: Trophozoites of Entamoeba histolytica/dispar with ingested erythrocytes
-
-
-
Primary Reference: Goldsmith, R. S., Antiprotozoal Drugs in Basic and Clinical Pharmacology (Katzung, B. G., ed) Appleton-Lange, 1998, p. 838-861.
Primary Reference: Morgan, Juliette and del Rio, Carlos, Amebiasis in Medicine for the Practicing Physician (Hurst, J. W., ed) Appleton-Lange, 1996, pp. 457-459.