Medical Pharmacology Chapter 43: Adult Cardiac Procedures
|
|
|
|
|
|
|
Medical Pharmacology Chapter 43: Adult Cardiac Procedures
|
|
|
|
|
|
|
Ventricular pressure, volume, ejection fraction information
Pulmonary pressures/resistances
Valvular luminal area estimates
Evaluation of shunts and determination of shunt flow magnitude
Determination of cardiac output and vascular resistance
Hemodynamic Status Assessment based on:
Focused historical interview (patient interview)
History of myocardial infarction; intermittent/chronic congestive heart failure
Congestive heart failure symptoms
fatigue
dyspnea on exertion
orthopnea
paroxysmal nocturnal dyspnea
ankle swelling
Physical exam (including evaluation of laboratory tests)
Hypotension/tachycardia (severe congestive failure)
Laterally displaced apical impulse
Prominent neck veins
Normal
S3 heart sound
S4 heart sounds
Rales
Pitting edema
An understanding of how current the information is.
Recognizing that certain factors have not yet been assessed, e.g. labile hypertension or arrhythmias.
Most Important Issue: Presence of heart failure (compensated or not): The major factor affecting surgical outcome:
Heart failure may influence
Anesthetic and related drug choices
Hemodynamic monitoring approaches
Severe heart failure results in patient in distress at rest (orthopneic short of breath, excesses sympathetic tone (pale, cold to the touch)): manage intraoperatively with significant caution because of limited cardiac reserve (poor ventricular function)
Indications of poor ventricular function
Enlarged Heart
Gallop rhythm: S3 heart sound, indicative of congestive heart failure (decompensation)
Veins: venous distention/engorgement; hepatojugular reflux
Edema: peripheral swelling; hepatomegaly; pneumonia; recurrent bronchitis, rales
Hypoperfusion-- manifestations
CNS effects: confusion
Renal effects: oligouria, abnormally high serum creatinine and blood urea nitrogen (BUN)
Muscle effects: fatigue
Cardiac effects: angina
Gastrointestinal/CNS: anorexia
Skin/mucous membranes: cyanosis and poor capillary filling
Hypotension (with exertion) is suggestive of reduced ventricular function due to ischemia.
4Risk Indicators from Nuclear Stress Imaging
Defect number (irreversible and reversible)
Severity of hypoperfusion (mild to severe)
Eevated lung/heart thallium uptake ratio
Left ventricular dilation induced by exercise.
"Abnormal nuclear perfusion images of left ventricular myocardium
(Top right) During stress, under perfused areas appear less bright (arrows) because of diminished radio tracer uptake.
(Bottom right) At rest, myocardium appears perfused, indicating reversible ischemia"
Zanger, D.R, Solomon, A.J., Gersh, BJ, Contemporary Management of Angina: Part I. Risk Assessment American Family Physician, December 1, 1999
Dyspnea: at rest, with exertion, nocturnal, orthopnea, associated with angina
Cardiac Function Tests:
Identification of ventricular dyskinesia, akinesis, hypokinesis, aneurysms)
Left ventricular end-diastolic pressures > 15 mm Hg
Ejection fraction < 0.5
Cardiac index < 2.5 liters/minute/meter2
4High Risk Indicators associated with Treadmill Exercise Stress Test
Exercise duration < 5 metabolic equivalents (1 metabolic equivalent = energy expended at rest)
ST-segment depression (see below)
Magnitude (>, = 2 mm)
Time of onset (stage I, II)
Duration (> 5 minutes)
ST segment depresssion observed in several ECG leads (>, = 5)
Blood Pressure
Low (< 130 mm Hg) peak systolic blood pressure
Decrease of systolic pressure to below initial resting standing blood pressure
Inability to attain target heart rate (target heart rate equals 85% of maximum predicted heart rate based on age (maximum predicted heart rate equals 220 - patients age)
Exercise-induced Angina
Ventricular ectopy (tachycardia/couplets) at low myocardial workload
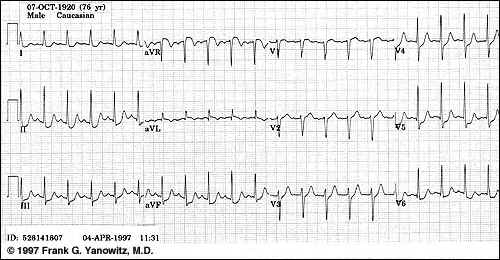
Electrocardiogram:
Arrhythmia-associated hemodynamic changes
Indications of ischemia/infarction
ST segmental depression
Acute:
may be associated with ischemia, non-Q wave infarction; hyperventilation, osmolality/electrolyte anomalies and drugs
ECG: obtain in patients with chest pain of unknown/uncertain etiology sense acute ST segmental shift may confirm ischemia (the amount of ST depression is measured from the PR segment (isoelectric line))
Chronic:
Non-specific cardiac disease marker -- associated with poor outcome
Causes: electrolyte abnormalities; drugs (e.g. digoxin (Lanoxin, Lanoxicaps)/digitoxin (Crystodigin))
Anatomical correlation: subendocardial damage (note that Q waves may be more likely associate with transmural infarction damage)
ST Segment Depression
"ST segment depression is a nonspecific abnormality that must be evaluated in the clinical context in which it occurs.
In a patient with angina pectoris ST depression usually means subendocardial ischemia and, unlike ST elevation, is not localizing to a particular coronary artery lesion."-Frank G.Yanowitz, M.D.
Dourtesy of: Frank G.Yanowitz, M.D. and The Alan E. Lindsey ECG Learning Center, used with permssion.
ST-segmental changes associated with myocardial ischemia, leads V4, V5, V6
Shaded areas indicate ECG changes associated was myocardial ischemia (possibly exercise into his, in this case associate with angina), adapted from the NIH publication No. 92-2890, U.S. Department of Health and Human Services, Public Health Service, National Institutes of Health, National Heart, long,and Blood Institute, April, 1994.
Cardiac Catherization: Information Concerning Patient's Cardiovascular Status
"Right Heart Catherization:Information"
Cardiac pressures
02 saturations
Cardiac output-thermal dilution or Fick principle
Systemic/pulmonary vascular resistance
Introcardiac shunt (congenital heart disorders)
Left atrial pressure estimate: derived from pulmonary capillary wedge pressure (PCWP)
"Left-heart Catherization -- angiographic information:
Method 1-- radioopaque contrast injected from a position above the aortic valve into the right and left coronary arteries which provides information concerning:
Location and degree of stenosis/stenoses
Method 2--radioopaque contrast injection from a catheter advanced past aortic valve and into the left ventricle: results in "left ventriculogram" which provides information concerning:
Ejection fraction
Ventricular wall motion anomalies
3D CT-based reconstructions of coronary arteries-courtesy GE Medical Systems
Left ventricular end diastolic pressure (LVEDP) may be measured both before and after contrast injection
significant LVEDP increased after injection is indicative of severe disease, since the contrast itself diminished function secondary to transient reduction in oxygen availability or by direct volume effects
Ventricular Functional Evaluation
Left ventricular end diastolic pressure (LVEDP) may be measured both before and after contrast injection
|
|
|
Left Image: diastole, A 6 French catheter is see in in the left ventricle (image was obtained at the end of diastole with maximal ventricular size and relaxation)
Right Image: systole-- minimal left ventricular size following ejection
Attribution: Cardiovascular Research Institute of Southern California, Ronald P. Karlsberg, M.D., Clinical and Interventional Cardiology, Associate Clinical Professor of Medicine, UCLA School of Medicine, used with permission
Significant LVEDP increased after injection is indicative of severe disease, since the contrast itself diminished function secondary to transient reduction in oxygen availability or by direct volume effects.
|
Good Ventricular Function |
Poor Ventricular Function |
|
|
Ventricular dysfunction may be indicated by some ventricular function measures but not others.
In this case focus should be placed on the unfavorable hemodynamic parameter come e.g. LVEDP of 20 mm Hg may suggest ventricular abnormality despite a normal cardiac output
5Ejection fraction-good indicator of myocardial function and surgical outcome (population: patients undergoing coronary artery bypass grafting procedures)
Ejection fraction > 0.4: best outcome i.e. Lowest mortality, morbidity, cost
Ejection fraction < 0.3: worse outcome
Ejection fraction between 0.3 and 0.39: intermediate outcome
Low ejection fraction, < 0.4 = significant ventricular dysfunction
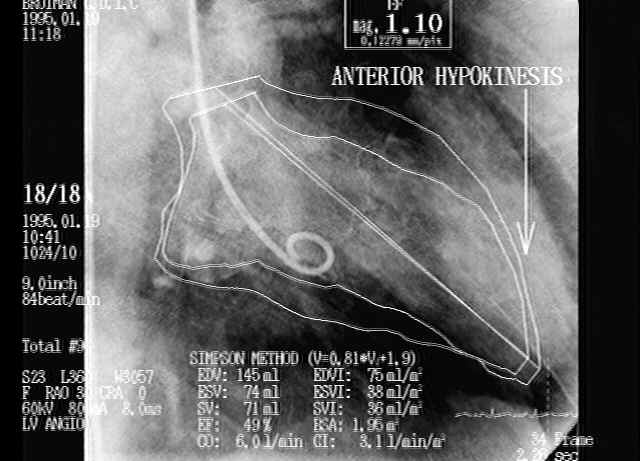
Ventricular dyskinesias: = significant ventricular dysfunction
Anterior wall myocardial dyskinesis/akinesis: more serious than similar findings associated with the inferior wall
Cardiac output may be normal even with low ejection fraction and dyskinetic regions in the presence of left ventricular aneurysm (ejection fraction is low due to systolic aneurysm region enlargement, but with sufficient remaining healthy myocardium, a normal cardiac output may be measured)
Diastolic phase superimposed on the systolic phase for ejection fraction calculation (percentage of blood volume that leaves the heart/beat); Cardiac regions with previous injury, i.e. scar tissue, are associated with impaired contractility (hypokinesis). In the example above, the anterior apical region exhibits reduced motion secondary to previous left anterior descending vessel occlusion.
Courtesy of: Cardiovascular Research Institute of Southern California, Ronald P. Karlsberg, M.D., Clinical and Interventional Cardiology, Associate Clinical Professor of Medicine, UCLA School of Medicine, used with permission.
Primary Reference: Ross, AF, Gomez, MN. and Tinker, JH Anesthesia for Adult Cardiac Procedures in Principles and Practice of Anesthesiology (Longnecker, D.E., Tinker, J.H. Morgan, Jr., G. E., eds) Mosby, St. Louis, Mo., pp. 1659-1698, 1998.
Primary Reference: Shanewise, JS and Hug, Jr., CC, Anesthesia for Adult Cardiac Surgery, in Anesthesia, 5th edition,vol 2, (Miller, R.D, editor; consulting editors, Cucchiara, RF, Miller, Jr.,ED, Reves, JG, Roizen, MF and Savarese, JJ) Churchill Livingston, a Division of Harcourt Brace and Company, Philadelphia, pp. 1753-1799, 2000.
Primary Reference: Wray Roth, DL, Rothstein, P and Thomas, SJ Anesthesia for Cardiac Surgery, in Clinical Anesthesia, third edition (Barash, PG, Cullen, BF, Stoelting, R.K, eds), Lippincott-Raven Publishers, Philadelphia, pp. 835-865, 1997
4Zanger, D.R, Solomon, A.J., Gersh, BJ, Contemporary Management of Angina: Part I. Risk Assessment American Family Physician, December 1, 1999
5Kay, GL, Sun, GW, Aoki, A, et al: Influence of ejection fraction on hospital mortality, morbidity, and costs for CABG patients, Ann. Thorac Surg 60 (6): 1640-1650, 1995 (2nd sourced from Ross, AF, Gomez, MN. and Tinker, JH Anesthesia for Adult Cardiac Procedures in Principles and Practice of Anesthesiology (Longnecker, D.E., Tinker, J.H. Morgan, Jr., G. E., eds) Mosby, St. Louis, Mo., pp. 201-218, 1998)
|
This Web-based pharmacology and disease-based integrated teaching site is based on reference materials, that are believed reliable and consistent with standards accepted at the time of development. Possibility of human error and on-going research and development in medical sciences do not allow assurance that the information contained herein is in every respect accurate or complete. Users should confirm the information contained herein with other sources. This site should only be considered as a teaching aid for undergraduate and graduate biomedical education and is intended only as a teaching site. Information contained here should not be used for patient management and should not be used as a substitute for consultation with practicing medical professionals. Users of this website should check the product information sheet included in the package of any drug they plan to administer to be certain that the information contained in this site is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. Advertisements that appear on this site are not reviewed for content accuracy and it is the responsibility of users of this website to make individual assessments concerning this information. Medical or other information thus obtained should not be used as a substitute for consultation with practicing medical or scientific or other professionals. |