Reduced transmitter
released affecting acetylcholine, norepinephrine, glutamate, serotonin,
substance P systems.
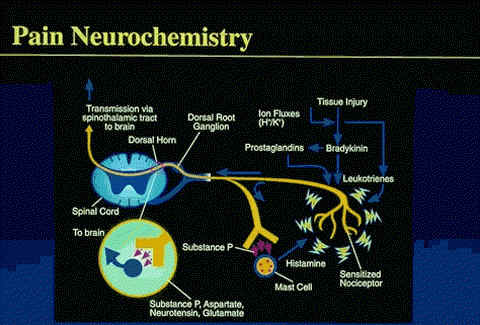
Serotonin, bradykinin, histamine,
prostaglandins, substance P (sP) , and various
ions (ie, H+ or K+), the biochemical mediators
released as a result of tissue injury, have been
implicated in nociceptive activation and
sensitization (hyperalgesia).
Hyperalgesia results in
enhancement of spontaneous pain via a reduction
in pain threshold and a lengthening in duration
of nociceptor response to stimuli.
PGE1, PGE2, and PGF2a, are the
most potent prostaglandins to produce these
sensitization effects.
Substance P, synthesized by cells
of the spinal ganglia, has been identified at the
peripheral terminal of unmyelinated primary
afferent fibers.
This putative neurotransmitter may
play a role in the propagation of visceral nociceptive pain from the gastrointestinal (GI)
tract, ureters, and urinary bladder.
In addition, to sP, other
potential nociceptive transmitters include
glutamate, aspartate, somatostatin,
cholecystokinin, and vasoactive intestinal
polypeptide.
courtesy of Roxane Pain Institute used
with permission
Way, W.L.,
Fields, H.L. and Way, E. L. Opioid Analgesics and
Antagonists, in Basic and Clinical
Pharmacology, (Katzung, B. G., ed)
Appleton-Lange, 1998, pp 496-515.
Schuckit, M.A.
and Segal D.S., Opioid Drug Abuse and Dependence, In
Harrison's Principles of Internal
Medicine 14th edition,
(Isselbacher, K.J., Braunwald, E., Wilson, J.D., Martin,
J.B., Fauci, A.S. and Kasper, D.L., eds) McGraw-Hill, Inc
(Health Professions Division), 1998, pp 2508-2512.
Coda, B.A. Opioids, In
Clinical Anesthesia, 3rd Edition
(Barash, P.G., Cullen, B.F. and Stoelting, R.K.,eds)
Lippincott-Ravin Publishers, Philadelphia, New York,
1997, pp 329-358.
Inhibit
excitatory transmitters
release from these
primary afferents
Inhibit
dorsal horn pain
transmission neurons
Clinical
application: directed administration of opioid
agonists allow regional
analgesia which minimizes
CNS side effects
"C Fibers are small, unmyelinated
nerves with slow conduction velocities that carry
dull, aching burning pain impulses.
Thinly myelinated A afferent
fibers carry fast, sharp, shooting pain
sensations and are most integral to the
propagation of mechanical pressure stimuli from
muscles, joints, and bone.
Compared with these fibers, C
afferent fibers have a higher threshold for
mechanical stimuli and a smaller field of
reception.
Both these classes of nociceptive
fibers ultimately synapse with neurons in the
dorsal horn of the spinal cord."
courtesy of Roxane Pain Institute used
with permission
"Transmission of impulses, which
as they reach consciousness will be interpreted as pain,
begins with the activation of specific peripheral
receptors called nociceptors by disease- or
surgery-induced tissue injury.
Nociceptors usually respond to high
intensity, potentially damaging stimuli.
Inflammatory processes often
associated with disease or tissue trauma play a role
in the initiation of nociception, mostly by
sensitizing the nociceptors:
which causes lowering of their
activation threshold.
Both A- and C-class nociceptors
and their corresponding afferent fibers are the most
important carriers of nociceptive stimuli from the
skin, deep somatic structures, such as muscle and
bone, and viscera.
On going nociceptor-evoked
discharges carried by these afferent fibers enter the
spinal cord via the dorsal roots, extending into
several ascending nociceptive pathways.
The dorsal horn is not only a
relay station for these signals, but also an area in
which complex data integration of excitatory or
inhibitory modulation occurs."
courtesy of Roxane Pain Institute used
with permission
Important opioid binding
sites in descending pathways
Rostral ventral
medulla
Locus ceruleus (see
below)
Midbrain
periaqueductal gray
Administration of exogenous
opioids promotes release of endogenous
opioids
adapted
from Figure 31-4: Way, W.L., Fields, H.L.
and Way, E. L. Opioid Analgesics and
Antagonists, in Basic
and Clinical Pharmacology, (Katzung, B. G., ed) Appleton-Lange,
1998, p. 505.