-
Introduction
-
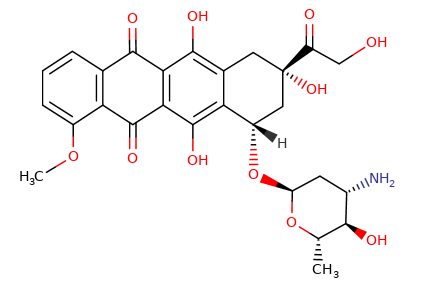
Epirubicin is an anthracycline
antibiotic and a stereoisomer of doxorubicin,
specifically the 4'-epimer [1].
-
This structural difference,
involving the orientation of the hydroxyl group
on the daunosamine sugar moiety, leads to
modifications in its pharmacological profile,
particularly concerning its metabolism and
toxicity, while largely retaining the anticancer
activity of doxorubicin [1, 2].
-
Epirubicin is widely used in the
treatment of various solid tumors and
hematological malignancies.
-
 Mechanism
of Action Mechanism
of Action
-
The
mechanisms by which epirubicin exerts its cytotoxic
effects are similar to those of other anthracyclines,
notably doxorubicin:
-
DNA Intercalation:
-
Epirubicin intercalates
between DNA base pairs, distorting the DNA
helix structure [2].
-
This physical binding interferes with
DNA replication and transcription,
hindering the synthesis of nucleic acids
and proteins, which are essential for
cell division and survival [3]
Topoisomerase II Inhibition:
-
Like doxorubicin, epirubicin
inhibits the enzyme topoisomerase II.
-
Epirubicin stabilizes the
covalent complex formed between
topoisomerase II and DNA (the "cleavable
complex"), which prevents the re-ligation
of DNA double-strand breaks created by
the enzyme during DNA replication and
transcription [3, 4].
-
The accumulation of these
unrepaired double-strand breaks triggers
cell cycle arrest and apoptosis.
-
Generation of Reactive Oxygen
Species (ROS):
-
Epirubicin can undergo redox
cycling, leading to the formation of
semiquinone free radicals and subsequent
generation of ROS, such as superoxide anions
and hydroxyl radicals [2].
-
These ROS can cause oxidative damage to DNA,
proteins, and cellular membranes,
contributing to its cytotoxicity.
-
Some
studies suggest that epirubicin may be taken up
by cells more rapidly and achieve higher
intracellular concentrations than doxorubicin,
potentially influencing its activity [1].
-
Pharmacokinetics (ADME)
-
Absorption:
-
Epirubicin is not orally
bioavailable and is administered intravenously
[6].
-
Distribution:
-
After IV administration,
epirubicin is rapidly and widely distributed
into body tissues, with a large volume of
distribution.
-
Epirubicin binds extensively to plasma
proteins.
-
Similar to doxorubicin,
its penetration into the central nervous
system (CNS) is poor [6, 7].
-
Metabolism:
-
Epirubicin is extensively
metabolized in the liver [7].
-
The main metabolic pathways include
reduction to epirubicinol (which has some
cytotoxic activity), cleavage of the
daunosamine sugar to form aglycones, and
conjugation (glucuronidation and sulfation)
[1, 7].
-
Epirubicin appears to be more
rapidly and extensively metabolized than
doxorubicin, which may contribute to its
faster clearance and potentially different
toxicity profile [1].
[12]
-
Metabolism:
-
Epirubicin is extensively
metabolized in the liver and also in other
tissues by cytoplasmic aldo-keto reductases [7,
13].
-
The main metabolic pathways include
reduction to epirubicinol (which has some
cytotoxic activity), cleavage of the
daunosamine sugar to form aglycones, and
conjugation (glucuronidation and sulfation)
[1, 7].
-
Epirubicin appears to be more
rapidly and extensively metabolized than
doxorubicin, which may contribute to its
faster clearance and potentially different
toxicity profile [1,12].
-
Clinical
Applications
-
Epirubicin is used in the treatment
of a range of cancers, often as part of combination
chemotherapy regimens.
Its approved indications can vary by region but may
include:
-
By far primary clinical use:
Breast cancer (both in adjuvant and metastatic
settings) [8]
-
Gastric
and esophageal cancer [8]
-
Ovarian
[14]
-
Lung
cancer (small cell)
[11]
-
Epirubicin is sometimes
preferred over doxorubicin in certain
regimens due to perceptions of a more
favorable toxicity profile, particularly
regarding cardiotoxicity at equi-effective
doses.
-
 Adverse Effects and Toxicities
Adverse Effects and Toxicities
-
The adverse
effect profile of epirubicin is qualitatively
similar to that of doxorubicin, but there are
quantitative differences, especially concerning
cardiotoxicity.
-
Cardiotoxicity:
-
Cardiotoxicity remains a
significant dose-limiting toxicity.
Like doxorubicin, epirubicin can cause both
acute (e.g., arrhythmias, transient ECG
changes) and chronic, cumulative
dose-dependent cardiomyopathy leading to
congestive heart failure [5, 9].
However, clinical data generally suggest
that epirubicin is less cardiotoxic than
doxorubicin on an equimolar or equieffective
dose basis.
The maximum recommended cumulative lifetime
dose for epirubicin is typically higher
(e.g., around 900 mg/m²) than that for
doxorubicin (450-550 mg/m²) before the risk
of cardiotoxicity becomes substantial [5,
9].
Cardiac function monitoring
is essential during treatment.
-
Myelosuppression:
-
Bone marrow
suppression, particularly neutropenia, is
the most common acute dose-limiting toxicity
[8].
Thrombocytopenia and anemia also occur.
The nadir is usually seen 10-14 days
post-administration.
-
Nausea and Vomiting:
-
Epirubicin is moderately to
highly emetogenic, often requiring
prophylactic antiemetics [8].
-
Alopecia:
-
Hair loss is common and often
complete [8].
-
Mucositis/Stomatitis:
-
Inflammation and ulceration
of the oral mucosa can occur.
-
Extravasation:
-
Epirubicin is a vesicant, and
extravasation during IV infusion can cause
severe local tissue injury and necrosis [6].
-
Secondary Malignancies:
-
There is an increased risk of
developing secondary cancers, such as acute
myeloid leukemia, following treatment with
epirubicin [8].
-
Red Discoloration of Urine:
-
Patients should be advised
that their urine may turn red for 1-2 days
after administration due to the drug's
color; this is a harmless effect [6].
-
Mechanisms
of Resistance
-
Resistance
to epirubicin is a significant clinical challenge
and shares mechanisms with doxorubicin resistance:
-
Increased Drug Efflux:
Overexpression of ATP-binding cassette (ABC)
transporters, such as P-glycoprotein (MDR1) and
Multidrug Resistance-associated Protein 1
(MRP1), actively pumps epirubicin out of cancer
cells, reducing its intracellular concentration
and efficacy [10].
-
Alterations in Topoisomerase II:
Decreased expression or mutations in the
topoisomerase II enzyme can reduce its
sensitivity to epirubicin [10].
-
Enhanced Detoxification:
Increased activity of detoxifying enzymes, like
glutathione S-transferases, can metabolize
epirubicin or scavenge the ROS it produces [10].
-
Defects in Apoptotic Pathways:
Alterations in cellular pathways that control
programmed cell death can render cells resistant
to epirubicin-induced damage [10].
-
Conclusion
-
Epirubicin is an important
anthracycline chemotherapeutic agent with a spectrum
of activity and mechanisms of action similar to
doxorubicin.
-
An important distinguishing feature is its
potentially more favorable cardiotoxicity
profile, which may allow for higher cumulative
doses and an improved therapeutic index in some
clinical settings.
-
Nevertheless, it still carries significant risks
of myelosuppression and other toxicities common
to anthracyclines.
-
Careful patient selection, dose management,
and monitoring are essential for its safe
and effective use in cancer treatment.
References
-
1.
Plosker, G. L.,
& Faulds, D. (1993). Epirubicin. A review of its
pharmacodynamic and pharmacokinetic properties, and
therapeutic efficacy in cancer. Drugs, 45(5),
788–856.
https://link.springer.com/article/10.2165/00003495-199345050-00011.
-
2.
Shandilya M Sharma S Das P Charak S Molecular-Level
Understanding of the Anticancer Action Mechanism of
Anthracyclines Advances in Precision Medicine Oncology
(H Arouk H and Hassan B, eds) 27 October 2020
https://www.intechopen.com/chapters/73668.
-
3. Tewey,
K. M., Rowe, T. C., Yang, L., Halligan, B. D., & Liu, L.
F. (1984).
Adriamycin-induced DNA damage mediated by mammalian DNA
topoisomerase II.
Science,
226(4673),
466–468.
https://pubmed.ncbi.nlm.nih.gov/6093249/ .
-
4.
Marinello J Delcuratolo M Capranico Anthracyclines as
Topoisomerase II Poisons: From Early Studies to New
Perspectives Int J Mol Sci 2018, 19(11), 3480
https://www.mdpi.com/1422-0067/19/11/3480
-
5.
Van Dalen, E. C., Michiels,
E. M., Caron, H. N., & Kremer, L. C. (2010). Different
anthracycline derivates for reducing cardiotoxicity in
children with cancer. Cochrane Database of
Systematic Reviews, (5), CD005006.
-
6. Robert, J. (1993). Clinical
pharmacokinetics of epirubicin. Clinical
Pharmacokinetics, 24(4), 275–287.
https://pubmed.ncbi.nlm.nih.gov/8070217/
-
7. Camaggi C Strocchi E Comparsi R
Testoni F Angelelli B Pannuti F
Biliary excretion
and pharmacokinetics of 4'epidoxorubicin (epirubicin) in
advanced cancer patients.
https://pubmed.ncbi.nlm.nih.gov/3463434/
8. Epirubicin
https://en.wikipedia.org/wiki/Epirubicin
9. Ryberg M Nielsen D et al.
Epirubicin
cardiotoxicity: an analysis of 469 patients with
metastatic breast cancer. Journal of Clinical Oncology
16(11) November 1, 1998.
https://ascopubs.org/doi/10.1200/JCO.1998.16.11.3502
10. Bukowski K Kciuk M Kontek Mechanisms
of Multidrug Resistance in Cancer Chemotherapy Int
J Mol Sci 2020, 21(9), 3233
https://www.mdpi.com/1422-0067/21/9/3233
11. Rosenthal M Kefford R Raghavan
D Stuart-Harris R
Epirubicin:
a phase II study in recurrent small-cell lung cancer
https://pubmed.ncbi.nlm.nih.gov/1713130/
12. Epirbicin: Package Insert
/ Prescribing Info (Drugs.com)
https://www.drugs.com/pro/epirubicin.html
13. Heibein A Sprowl AJ MacLean DA
Parissenti
Abstract 3546: Role of the “1C” Aldo-Keto Reductases in
Resistance to Doxorubicin in MCF-7 breast cancer cells
Cancer Res (2010)
70 (8_Supplement): 3546
https://aacrjournals.org/cancerres/article/70/8_Supplement/3546/564127/Abstract-3546-Role-of-the-1C-Aldo-Keto-Reductases
14.
Havsteen H Bertelsen K et al.
A phase 2 study
with epirubicin as second-line treatment of patients
with advanced epithelial ovarian cancer Gynecol Oncol
1996 Nov; 63(2): 210-215.
https://pubmed.ncbi.nlm.nih.gov/8910629/
|