|
|
|
|
|
|
|
Medical Pharmacology Chapter 33-34: Anticancer Drugs
|
|
|
|
|
|
|
Miscellaneous Anticancer Drugs:
References
|
||
Mitomycin (Mitosol)
|
|
Mitomycins refer to a group of aziridine-containing natural products which are obtained from either Streptomyces caespitosus or Streptomyces lavendulae.10
The group consists of mitomycin A, mitomycin B, and mitomycin C.
The use of the term "mitomycin" alone usually refers to mitomycin C which is used clinically.10
|
|
|
Mitomycin (mitomycin C, Mitosol) is classified as an antibiotic anticancer drug.3
This antibiotic was first isolated from Streptomyces caespitosus in 1958.3,8
Mitomycin is a prodrug requiring metabolic activation which, by means of a cytochrome P450-dependent enzyme catalyzed reduction, results information of a DNA cross-linking agent (alkylating agent).3,9
Hypoxic tumor stem cells associated with solid tumors tend to be hypoxic which results in an environment that promotes reductive reactions.
As a result, the cells tend to be more responsive to mitomycin cytotoxicity compared to normal cells or even the more oxygenated tumor cells.
Mitomycin is an effective antineoplastic agent in all phases of the cell-cycle and appears particularly efficacious when combined with radiation treatment directed at hypoxic tumor.
![]() At present,
this
agent is primarily used in combination treatment for anal squamous cell
cancer.
At present,
this
agent is primarily used in combination treatment for anal squamous cell
cancer.
Mitomycin is combined with 5-fluorouracil and radiation in this setting.3
Absorption, Distribution, Biotransformation, Excretion:
Mitomycin is administered by the IV (intravenous) route of administration, exhibiting a t½ of about 25-90 minutes.1
Mitomycin is widely distributed throughout the body but is not found in the central nervous system1
Mitomycin undergoes liver metabolism and is mainly excreted in the feces and to a lesser extent in urine (10%) .1,6
Additionally, mitomycin may also be inactivated through chemical conjugation with sulfhydryl groups.1
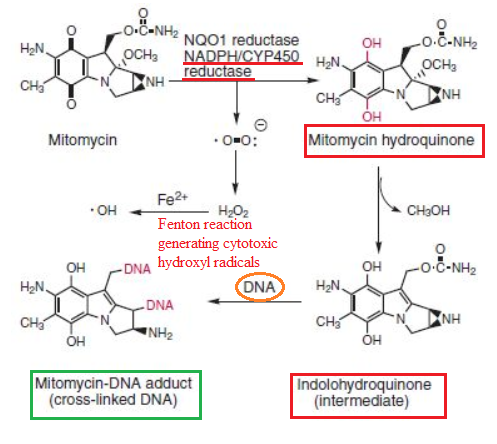
As noted earlier, mitomycin is a "prodrug" and therefore requires activation to exert its antineoplastic activity.
This process involves NADPH/Cytochrome P450 reductase catalyze conversion of mitomycin to mitomycin hydroquinone with subsequent formation of indolohydroquinone.
This latter form interacts with DNA, forming the cross-linked DNA mitomycin-DNA adduct.9
This sequence is shown below, adapted from reference 9, Figure 37.27.
|
|
|
The principal clinical use of mitomycin is in the treatment of anal squamous cell carcinoma.14
Mitomycin is combined with 5-FU (5-fluorouracil) and radiation.
Anal canal carcinoma represents a rare malignancy in the United States.
This carcinoma has limited metastatic potential (about 15%), making it a "local-regional" cancer.
![]() When
chemotherapy is used along with radiation, cure rates approximate 60%,
depending on the initial primary tumor size.
When
chemotherapy is used along with radiation, cure rates approximate 60%,
depending on the initial primary tumor size.
![]() Five-year
survival rates fall substantially for tumors greater than 5 cm in diameter.
Five-year
survival rates fall substantially for tumors greater than 5 cm in diameter.
A reduction in cure rate is also associated with nodal metastases.
Standard treatment involves mitomycin (along with 5-FU and radiation); however, substituting cisplatin results in a comparable disease-free-survival time but with the significantly worse colostomy rate.14
![]() Advanced,
Metastatic Anal Cancer
Advanced,
Metastatic Anal Cancer
|
Superficial "transitional cell" carcinomas of the bladder may also be treated using mitomycin, by direct installation into the bladder.1
![]() Metastatic
Bladder Cancer:
Metastatic
Bladder Cancer:
|
Other clinical uses of mitomycin include:3
Combined with other chemotherapy drugs for cervical squamous cell carcinoma
Breast cancer
Gastric cancer
Pancreatic cancer3
![]() The major
adverse, toxic reaction to mitomycin administration is myelosuppression.
The major
adverse, toxic reaction to mitomycin administration is myelosuppression.
This myelosuppression is associated both with significant leukopenia and thrombocytopenia.
Myelosuppression may be both delayed and cumulative with an extended recovery time that may include 6-8 weeks of pancytopenia.1
Other adverse effects include1 :
Stomatitis
Nausea
Diarrhea
Vomiting
Rash Fever.
At higher doses (>50 mg/m2) a patient may be at risk for:1
Hemolysis
Interstitial pneumonia
Neurological dysfunction
Renal failure, secondary to glomerular damage.
At the higher doses, 70 mg/m2 about 28% of patients may experience renal failure.1
A "Hemolytic-Uremic Syndrome" has been identified, presenting as microangiopathic hemolytic anemia, along with thrombocytopenia and renal failure.3
This syndrome
may, on occasion, present with interstitial pneumonitis.3
|
|
|
|
|
|
|