|
|
|
|
|
|
|
Medical Pharmacology Chapter 33-34: Anticancer Drugs
|
|
|
|
|
|
|
Hormonal Anticancer Drugs:
Overview: Cytochrome P450 enzyme, CYP17 inhibitor5
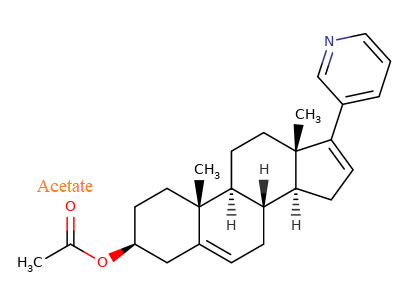
Abiraterone acteate5 (Zytiga: abiraterone acetate + prednisone; Yonsa: abiraterone acetate + methylprednisolone)
![]() Abiraterone
acetate is classified as an anti-androgen agent given that it prevents or
limits formation of testosterone precursors: dehydroepiandrosterone (DHEA)
and anthracenedione.
Abiraterone
acetate is classified as an anti-androgen agent given that it prevents or
limits formation of testosterone precursors: dehydroepiandrosterone (DHEA)
and anthracenedione.
The mechanism of action involves a selective and a reversible inhibition of a cytochrome P450 enzyme, CYP17 (17 α-hydrolase/C17,20-lyase).
CYP17 is an enzyme essential for catalysis of androgen biosynthesis.
The enzyme is found in testicular, adrenal and prostate cancer cells. abiraterone acetate is typically combined with prednisone or methylprednisolone.
![]() Abiraterone
acetate is a steroidal prodrug which is converted into an active 3β-hydroxy
metabolite in esterase-catalyzed reactions1 .
Abiraterone
acetate is a steroidal prodrug which is converted into an active 3β-hydroxy
metabolite in esterase-catalyzed reactions1 .
Abiraterone is typically combined with prednisone in treating castration-resistant prostate cancer (CRPC) patients who have not previously received chemotherapy or who have received previous docetaxel1 .
Following castration, androgen receptor signaling even though steroid levels are low continues to promote prostate cancer cell proliferation.
Androgen receptor activation may result from binding of androgens produced from nongonadal sources or as a result of androgen receptor (AR) genetic mutations or amplifications.
Examples of nongonadal androgen sources include adrenal glands and prostate cancer cells.
For instance, anthracenedione synthesized in adrenal glands is transformed to testosterone in tumors and peripheral tissues.1
![]() The rationale
of using androgen synthesis inhibitors is their ability to counteract
androgen receptor activation in the castrate state.1
The rationale
of using androgen synthesis inhibitors is their ability to counteract
androgen receptor activation in the castrate state.1
Abiraterone acetate (FDA approval, 2011) administered for treatment of metastatic castration resistant prostate cancer (mCRPC) following docetaxel treatment extended survival by about four months.6
|
|
|
|
|
Absorption, Distribution, Biotransformation, Excretion
![]() Abiraterone is administered orally, typically in combination with
prednisone in order to limited adrenal suppression.
Abiraterone is administered orally, typically in combination with
prednisone in order to limited adrenal suppression.
This agent should be preferably taken on an empty stomach.1
Maximal plasma concentration of the active agent abiraterone, following oral administration of abiraterone acetate, occurs in about two hours following administration.10
Given the poor drug solubility, the presence of food significantly and inconsistently alters drug absorption.
For example, consumption of low-fat food increases absorption by about 6 times.10
By contrast, consumption of a high-fat meal may increase absorption up to 17 times.
Accordingly, food should not be consumed within one hour before or 2 hours after abiraterone administration.10
Bioavailability appears to be increased by food resulting in higher systemic drug levels.10
Abiraterone is substantially bound (greater than 99% to plasma proteins, albumin as well as α-1 acidic glycoprotein.12
The steady-state volume of distribution (apparent) is about 19,000 +/- 13,000 L (mean +/- s.d.)12
This large volume of distribution (Vd) is indicative of very poor solubility.10
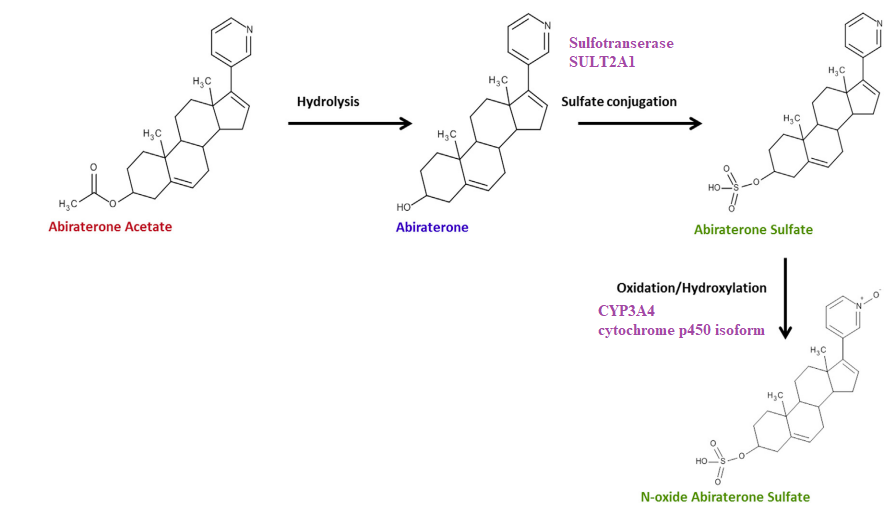
Following activation from the prodrug precurser abiraterone acetate, abiraterone is subject to metabolism.
The major circulating abiraterone metabolites are sulfate derivatives: abiraterone sulfate and N-oxide abiraterone sulfate.
Abiraterone sulfate formation is catalyzed by sulfotransferase family 2A Member 1 (SULT2A1); whereas, the N-oxide abiraterone sulfate is formed in a reaction catalyzed by the cytochrome P450 isoform CYP3A4.10
|
|
|
Excretion:10
Elimination half-life is about 15 hours typically. However, in
patients with some hepatic impairment extended half-life of
elimination is noted (18-19 hours).10
Following oral dosing (in a population of castration resistant
prostate cancer patients), most of the administered agent is
recovered in the feces as unchanged abiraterone acetate (55%) and
abiraterone (22%).10,14
An additional 5% is found in the urine.14
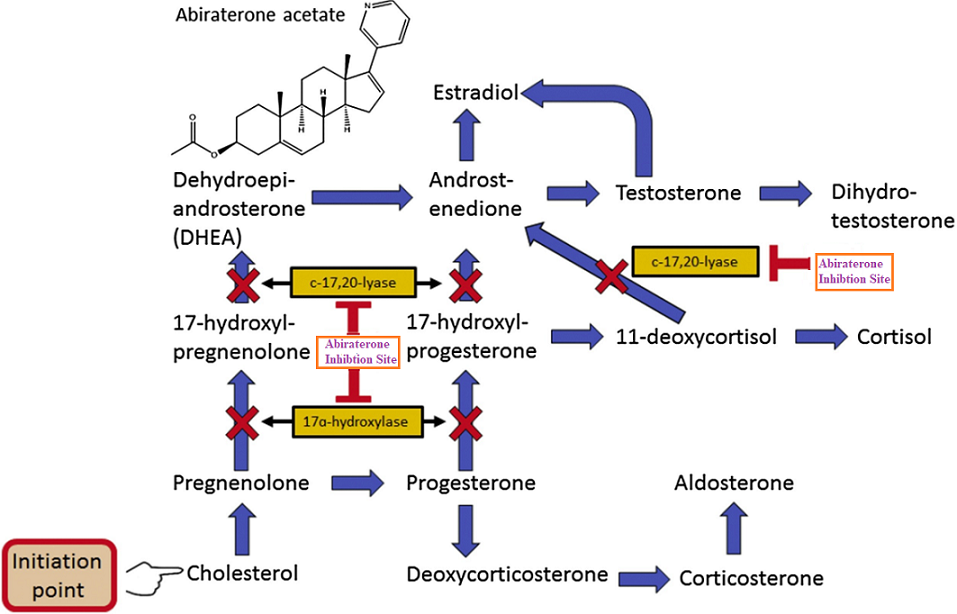
Abiraterone reversibly inhibits both 17α-hydroxylase and C-17,20-lyase (CYP17A1) enzymatic activity in:
Testicular
Adrenal, and
Prostate cancer tissue.
CYP17A1 inhibition:
Decreases pregnenelone and progesterone conversion to their corresponding 17 α-hydroxy derivatives and
Decreases DHEA (dehydroepiandrosterone) synthesis and
Decreases androstenedione synthesis.
 |
|
Initially, abiraterone was FDA approved for use in management of metastatic castration-resistant prostate cancer, as secondary hormonal treatment.
A clinical study, "Cougar-301" compared clinical results in patients previously having received chemotherapy with docetaxel to treatment with abiraterone acetate with prednisone or placebo.
The result indicated that abiraterone compared to placebo conferred an improved overall survival (14.8 months versus 10.9 months).
Abiraterone was also shown to be associated with overall improved survival when comparing patients, not having received prior docetaxel chemotherapy, but receiving either placebo or abiraterone acetate with prednisone.
In 2017 clinical trial results indicated a role for abiraterone acetate in management of metastatic castration-sensitive prostate cancer. In these studies ("LATITUDE") patients began androgen deprivation therapy and after three months either androgen deprivation therapy (ADT) was continued as sole therapy or abiraterone acetate with prednisone was added.
Addition of abiraterone improved overall survival.
![]() Accordingly,
in many men with metastatic castration-sensitive prostate
cancer, newly diagnosed, standard of care involves
combination of androgen deprivation therapy with abiraterone
acetate or docetaxel.11
Accordingly,
in many men with metastatic castration-sensitive prostate
cancer, newly diagnosed, standard of care involves
combination of androgen deprivation therapy with abiraterone
acetate or docetaxel.11
|
Hepatotoxicity |
Joint Swelling |
Low Potassium |
Diarrhea |
Cough |
|
Vasomotor symptons |
Urinary Frequency |
Dyspepsia |
Upper Respiratory Tract Infection |
Arrhythmia |
Many of the above side effects are related to the principal abiraterone acetate toxicity, mineralocorticoid excess.
These toxicities include:
Hypertension
Fluid excess, and
Hypokalemia.
Blockade of the cytochrome P450 isoform CYP17A1 results in increased adrenocorticotropic hormone (ACTH).
This increase in ACTH increases level of corticosterone and deoxycorticosterone.
Coadministration of steroids may mitigate adverse effects.
|
|
|
|
|
|
|