![]()
![]()
|
|
Anesthesia Pharmacology Chapter 20: Renal Pharmacology
![]()
![]()
|
|
|
|
Background:
Body fluid and electrolyte composition are regulated by the kidney-- drugs that interfere with renal transport may be useful in management of clinical disorders.
Diuretics are drugs which block renal ionic transport, causing diuresis {an increase in urine volume}, often associated with natriuresis {increase in sodium excretion}
Diuretics often act at different sites of the tubule transport system, at specific membrane transport proteins
Diuretics that act on specific membrane transport proteins include:
loop diuretics
thiazides
amiloride (Midamor)
triamterene (Dyrenium)
Diuretics may act through:
osmotic effects (preventing water reabsorption)-- mannitol
enzyme inhibition (carbonic anhydrase inhibitor)-- acetazolamide
interaction with hormonal receptors: spironolactone
Renal physiology and sites of diuretic action:
|
courtesy of Robert H. Parsons, Ph.D., Rensselaer Polytechnic Institute, used with permission |
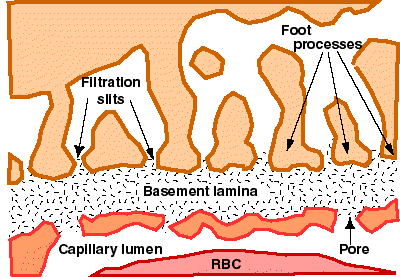 |
"The glomerular capillaries are very leaky about 400 times as high as most other capillaries and produce a filtrate that is similar to blood plasma except the it is devoid of proteins and cellular elements.
The glomerular filtration rate (GFR) is effected by the same forces as other capillaries:
GFR = Kf X (Pc -Pb - PiG +PiB)
where Kf = Filtration coefficient
Pc = Glomerular hydrostatic pressure
Pb = Bowman's capsule hydrostatic pressure
PiG = Glomerular capillary colloidal osmotic pressure
PiB = Bowman's capsule colloidal osmotic pressure "
courtesy of Robert H. Parsons, Ph.D., Rensselaer Polytechnic Institute, used with permission
Many solutes are reabsorbed in the early portions of the proximal tubule:
85% of filtered sodium bicarbonate
40% of sodium chloride
60% of water
nearly all of filtered organic solutes, including glucose and amino acids
glucose, amino acids, and other organic solutes are reabsorbed by specific transport systems
Mechanism of Action: In the proximal tubule, sodium bicarbonate reabsorption can be influenced by carbonic anhydrase inhibitors.
Sodium bicarbonate reabsorbed in the proximal tubule depends on the action of sodium/hydrogen exchanger which is found in the luminal membrane of the proximal tubule epithelial cell.
proton secreted into lumen (urine) combine with bicarbonate to form carbonic acid (H2CO3)
Carbonic acid is dehydrated by an enzyme carbonic anhydrase which is localized (among other places) on the brush border membrane.
The dehydration products carbon dioxide and water easily move across membranes. Carbon dioxide enters the proximal tubule by diffusion where it is rehydrated back to carbonic acid.
Carbonic acid dissociates back to bicarbonate and the proton (step one)
This cycle depends on carbonic anhydrase
Mechanism of Action: Inhibition of carbonic anhydrase decreases bicarbonate reabsorption in proximal tubule, which in turn decreases water reabsorption
Carbonic anhydrase inhibitor: acetazolamide (Diamox)
In the proximal tubule, water is reabsorbed in direct proportion to salt.
With a large concentration of impermeant solute, such as glucose or the diuretic mannitol, water reabsorption would decrease for osmotic reasons. (Mechanism for osmotic diuresis)
Located in the middle third proximal tubule
Organic acid secretory system secretes for example:
uric acid
antibiotics
p-aminohippuric acid
Localized in both early and middle segments of the proximal tubule
Organic base secretory system secretes, for example:
creatinine
procainamide {antiarrhythmic drug}
choline
Organic acid and base transport systems are important in delivery of diuretics to their site of action: luminal side
Drug interaction: diuretics and probenecid (secretory system inhibitor)
water reabsorption
driving force: osmotic -- due to hypertonic medullary fluid
no active salt reabsorption, but impermeant solutes (mannitol, glucose) will inhibit water reabsorption {a site of action for osmotic diuretics}
Thick ascending limb of the loop of Henle: active sodium chloride reabsorption {about 35% of filtered load}--
impermeable to water
since reabsorption of sodium chloride at this site dilutes the fluid in the tubule, this segment may be referred to as "diluting segment."
Reabsorption of sodium chloride in the thick ascending limb is dependent upon the Na/K/2Cl co-transporter.
Loop diuretics block this transporter.
furosemide (Lasix)
bumetanide (Bumex)
ethacrynic acid (Edecrin)
torsemide (Demadex)
Normal activity of this transporter and Na/K ATPase results in an increase in intracellular potassium, potassium efflux, and a lumen-positive electrical potential:
This lumen-positive membrane potential provides the driving force for reabsorption of magnesium and calcium cations.
Therefore loop diuretics which inhibit the action of the sodium potassium chloride co-transporter, leading to increase sodium excretion also leads to increased magnesium and calcium loss.
Properties:
impermeable to water
sodium reabsorption (about 10% of filtered load) by sodium and chloride co-transporter
further dilution of tubular fluids
Pharmacological blockade of sodium and chloride co-transporter:
thiazide diuretics
no potassium recycling; no lumen-positive membrane potential; -- no calcium or magnesium loss by electrical forces
Calcium is actively reabsorbed by:
an apical calcium channel and
Na/Ca exchanger
regulated by parathyroid hormone
Properties:
About 2% to 5% of sodium chloride reabsorption
Final site for sodium chloride reabsorption -- responsible for final sodium concentration in the urine
This site and late distal tubule -- where mineralocorticoids exert their effect
Major site of potassium secretion
Major sites for sodium, potassium, and water transport
principal cells
Major site for proton secretion -- intercalated cells
Separate sodium and potassium channels:
Significant driving force for sodium entry
Na after entering the principal cell is transported to the blood {Na/K ATPase} with potassium translocated to the lumen urine (lumen-negative electrical potential drives chloride back to the blood)
Accordingly, delivery of increased sodium to the collecting tubule drives increased potassium efflux
Diuretics (acting upstream) that increased delivery of sodium to the collecting tubule will cause potassium loss
Delivery of bicarbonate {not readily reabsorbed compared chloride, increasing lumen-negative potentials}, will increase further potassium loss.
Diuretic-induced potassium loss, which is clinically important, results from the above mechanisms coupled with enhanced aldosterone secretion due to volume depletion.
Major pharmacokinetic, pharmacodynamic and mechanism of action of Diuretic Classes:
Carbonic Anhydrase Inhibitors
Potassium Sparing
Loop Diuretics
Thiazides
Osmotic Agents
The enzyme, carbonic anhydrase exhibits the following characteristics:
Its major location is the luminal proximal tubule membrane.
Carbonic anhydrase catalyzes dehydration of carbonic acid, H2CO3 , required for bicarbonate reabsorption
Blockade of carbonic anhydrase activity induces a sodium bicarbonate diuresis, which reduces body bicarbonate levels
Carbonic anhydrase inhibitors are unsubstituted sulfonamides which are bacteriostatic. These agents promote alkaline diuresis and a hyperchloremic metabolic acidosis.
Prototype drug: acetazolamide (Diamox)
Acetazolamide: (Diamox) is well absorbed orally and is excreted by tubular secretion, at the proximal tubule.
In renal insufficiency a dose reduction is appropriate.
At maximal carbonic anhydrase inhibition, a 45% inhibition of bicarbonate reabsorption is observed.
This level of inhibition results in significant bicarbonate loss and a hyperchloremic metabolic acidosis.
Acetazolamide (Diamox) administration causes a reduction in aqueous humor and cerebrospinal fluid production
Glaucoma:
Because acetazolamide decreases the rate of aqueous humor production, a decline in intraocular pressure occurs.
Management of glaucoma is the most common indication for use of carbonic anhydrase inhibitors.
Dorzolamide (Trusopf), another carbonic anhydrase inhibitor exhibits no diuretic or systemic metabolic effect; however, administration of this agent causes a reduction in intraocular pressure.
Urinary Alkalinization:
increased uric acid and cystine solubility by alkalinizing the urine (by increasing bicarbonate excretion)
for prophylaxis of uric acid renal stones, bicarbonate administration (baking soda) may be required
Metabolic Alkalosis:
Results from:
decreased total potassium with reduced vascular volume
high mineralocorticoid levels
These conditions are usually managed by treating the underlying causes; however, in certain clinical settings acetazolamide may assist in correcting alkalosis {e.g. alkalosis due to excessive diuresis in CHF patients}
Acute Mountain Sickness:
Symptoms: weakness, insomnia, headache, nausea, dizziness {rapid ascension of all of 3000 meters}; symptoms -- usually mild
In serious cases: life-threatening cerebral or pulmonary edema
Acetazolamide reduces the rate of CSF formation and decreases cerebral spinal fluid pH.
Prophylaxis against acute mountain sickness may be appropriate
Other Uses:
some role in management of epilepsy
hypokalemia periodic paralysis
increase urinary phosphate excretion during severe hyperphosphatemia.
Toxicity:
hyperchloremic metabolic acidosis
due to reduction of body bicarbonate stores
renal stones:
bicarbonate loss is associated with:
phosphaturia
hypercalciuria (calcium salts, relatively insoluble at alkaline pH)
renal potassium loss:
increased sodium bicarbonate in the collecting tubule increases the lumen-negative electrical potential -- enhances potassium excretion
counteracted by potassium chloride administration
Others:
drowsiness, parathesias
accumulation in renal failure (CNS toxicity)
hypersensitivity reactions
Contraindications:
hepatic cirrhosis
urinary alkalinization will decrease ammonium ion trapping, increasing the likelihood of hepatic encephalopathy.
Agents include:
furosemide (Lasix)
bumetanide (Bumex)
torsemide (Demadex)
ethycrinic acid --no longer in use because of toxicity.
inhibition of NaCl reabsorption in the thick ascending limb of the loop of Henle
inhibit the Na/K/2Cl transport system in the luminal membrane
reduction in sodium chloride reabsorption
decreases normal lumen-positive potential (secondary to potassium recycling)
Positive lumen potential: drives divalent cationic reabsorption (calcium magnesium)
Therefore, loop diuretics increase magnesium and calcium excretion.
hypomagnesemia may occur in some patients.
hypocalcemia does not usually develop because calcium is reabsorbed in the distal convoluted tubule.
{in circumstances that result in hypercalcemia, calcium excretion can be enhanced by administration of loop diuretics with saline infusion}
Since a significant percentage of filtered NaCl is absorbed by the thick ascending limb of loop of Henle, diuretics acting at this site are highly effective
Loop diuretics--Properties: rapidly absorbed following oral administration (may be administered by IV)
acts rapidly
eliminated by a renal secretion and glomerular filtration (half-life -- depend on renal function)
co-administration of drugs that inhibit weak acid secretion (e.g. probenecid or indomethacin) may alter loop diuretic clearance.
Other effects:
Furosemide: increases renal blood flow; blood flow redistribution within the renal cortex
Furosemide decreases pulmonary congestion and the left ventricular filling pressure in congestive heart failure (CHF) -- prior to an increase in urine output.
Other uses:
loop diuretics increase potassium excretion
effect increased by concurrent administration of NaCl and water.
may increase rate of urine flow and increase potassium excretion.
may convert oligouric to non-oligouric failure {easier clinical management}
renal failure duration -- not affected
bromide, chloride, iodide: all reabsorbed by the thick ascending loop:
systemic toxicity may be reduced by decreasing reabsorption
concurrent administration of sodium chloride and fluid is required to prevent volume depletion
Hypokalemia metabolic alkalosis:
increased delivery of NaCl and water to the collecting duct increases potassium and proton secretion-- causing a hypokalemic metabolic alkalosis
in managed by potassium replacement and by ensuring adequate fluid intake
dose-related hearing loss (in usually reversible)
ototoxicity more common:
with decreased renal function
with concurrent administration of other ototoxic drugs such as aminoglycosides
may cause gout
loop diuretics cause increased uric acid reabsorption in the proximal tubule, secondary to hypovolemic states.
Hypomagnesemia: loop diuretics cause:
reduction in sodium chloride reabsorption
decreases normal lumen-positive potential (secondary to potassium recycling)
Positive lumen potential: drives divalent cationic reabsorption (calcium magnesium)
Therefore, loop diuretics increase magnesium and calcium excretion.
hypomagnesemia may occur in some patients.
reversed by oral magnesium administration
furosemide: skin rash, eosinophilia, interstitial nephritis(less often)
Other toxicities:
Dehydration (may be severe)
hyponatremia (less common than with thiazides thought may occur in patients who increased water intake in response to a hypovolemic thirst)
Hypercalcemia may occur in severe dehydration and if a hypercalcemia condition {e.g. oat cell long carcinoma} is also present.
Ives, H.E., Diuretic Agents, in: Basic and Clinical Pharmacology, (Katzung, B. G., ed) Appleton-Lange, 1998, pp 242-259.
Introduction:
Thiazides inhibit NaCl transport at the distal convoluted tubule
Prototypical thiazide: hydrochlorothiazide
|
bendroflumethazide |
benzthiazide |
chlorothiazide |
chlorthalidone |
|
hydrochlorothiazide |
hydroflumethiazide |
indapamide |
methyclothiazide |
|
metolazone |
polythiazide |
quinethazone |
trichlomethiazide |
Properties:
Oral administration
Secreted by the organic acid secretory system
compete with uric acid for secretion {uric acid secretory rates may decline}
Differences between thiazides:
chlorothiazide (Diuril): less lipid soluble (requires relatively large doses)
chlorthalidone (Hygroton): slowly absorbed -- longer duration of action
indapamide (Lozol): mainly biliary secretion
Mechanism of action:
Diuretic action:Inhibition of NaCl reabsorption from the distal convoluted tubule (luminal side)
enhance calcium reabsorption in the distal convoluted tubule (unknown mechanism)
thiazides infrequently cause hypercalcemia but can unmask hypercalcemia due to other causes such as carcinoma, sarcoidosis, or hyperparathyroidism.
Clinical Uses:
Hypertension
Congestive heart failure
Nephrolithiasis (due to idiopathic hypercalciuria
Nephrogenic diabetes insipidus
Toxicity:
Hypokalemic metabolic alkalosis and hyperuricemia
Impaired carbohydrate tolerance
may induce hyperglycemia
impaired pancreatic insulin release
decreased tissue glucose utilization
hyperglycemia may be partially reversed by correcting a hypokalemic state
Hyperlipidemia
5% to 15% increase in serum cholesterol and an increase in low-density lipoproteins.
Hyponatremia:
Significant adverse effect, occasionally life-threatening
Mechanism:
hypovolemia-induced increase in ADH
reduced renal diluting capacity
increased thirst
Prevention: decreasing the drug dose or limiting fluid intake
Allergic reactions:
Thiazides are sulfonamides: cross-reactivity within the group
photosensitivity {rare}
dermatitis {rare}
Extremely rare reactions:
hemolytic anemia
thrombocytopenia
acute necrotizing pancreatitis
Other reactions:
weakness
fatigue
paresthesias
Potassium-Sparing Diuretic Agents
Introduction:
These diuretics inhibit the effects of aldosterone at the cortical collecting tubule and late distal tubule.
Mechanisms of action:
In the collecting tubule and duct, sodium reabsorption and potassium excretion is regulated by aldosterone.
Aldosterone increases potassium secretion by increasing Na/K ATPase activity and sodium and potassium channel activity.
Normally, sodium absorption in the collecting tubule results in a lumen-negative electrical force that drives potassium excretion.
Aldosterone antagonists interfere with this effect
Aldosterone antagonists act similarly with respect to proton movement, accounting for metabolic acidosis associated with aldosterone antagonists.
pharmacologic antagonism at mineralocorticoid receptors { spironolactone (Aldactone)}
inhibition of sodium transport through the luminal membrane {triamterene (Dyrenium), amiloride (Midamor)}
Some Potassium-Sparing effects occur with nonsteroidal anti-inflammatory drugs, beta-blockers, converting enzyme-inhibitors, and angiotensin receptor blockers.
Spironolactone (Aldactone):
Synthetic steroid: competitive aldosterone antagonist
binds to cytoplasmic mineralocorticoid receptors -- preventing receptor complex translocation to the nucleus
also inhibits formation of active metabolite of aldosterone {by inhibiting 5-alpha reductase activity}
hepatic inactivation
slow onset of action
Triamterene (Dyrenium):
Renal excretion; hepatic metabolism-- extensive metabolism (short half life)
Directly blocks Na entry through sodium-specific channels (apical collecting tubule membrane) -- note that since potassium secretion is coupled to sodium entry, potassium secretion {potassium-sparing} is reduced.
Amiloride (Midamor):
Excreted unchanged (urine)
Directly blocks Na entry through sodium-specific channels (apical collecting tubule membrane) -- note that since potassium secretion is coupled to sodium entry, potassium secretion {potassium-sparing} is reduced.
Clinical Uses:
Mineralocorticoid excess:
Conn's syndrome (primary hypersecretion)
ectopic ACTH production (primary hypersecretion)
secondary aldosteronism caused by:
congestive heart failure
hepatic cirrhosis
nephrotic syndrome
conditions that cause renal salt retention with reduced intravascular volume
other diuretics may further reduce intravascular volume thus worsening secondary aldosteronism
Toxicity:
Hyperkalemia:
Potassium-sparing diuretics can cause significant hyperkalemia
Factors that increase the likelihood of hyperkalemia:
renal disease
presence of agents that reduce renin:
beta-blockers
nonsteroidal anti-inflammatory drugs (NSAIDs)
ACE inhibitors
angiotensin receptor blockers
hyperkalemia more likely when potassium-sparing diuretics are used as the only diuretic drug or in the presence of renal insufficiency.
given in combination with thiazides, hypokalemia and metabolic alkalosis associated with thiazide use may be balanced by aldosterone antagonists
Since thiazide adverse effects may predominate {hyponatremia, metabolic alkalosis}, due to variations in bioavailability, individual dose adjustment of the two drugs may be better.
Hyperchloremic Metabolic Acidosis:
Acidosis cause by inhibition of proton secretion along with potassium secretion {similar to type IV renal tubular acidosis
Gynecomastia:
Endocrine abnormalities associated with synthetic steroids --Spironolactone (Aldactone)
gynecomastia (breast enlargement)
impotence
benign prostatic hyperplasia
Acute Renal Failure:
Triamterene (Dyrenium) plus indomethacin
Kidney Stones:
Triamterene (Dyrenium) (poorly soluble) may precipitate in urine, causing renal stones:
Contraindications:
may cause severe (potentially fatal) hyperkalemia
potassium supplements should be discontinued prior to administration of aldosterone antagonists
patients with chronic renal insufficiency are at particular risk
hyperkalemia is also more likely to occur or it if beta-blockers or ACE inhibitors are concurrently administered
impairment of hepatic metabolism of triamterene spironolactone may require dose adjustment
Introduction:
Osmotic diuretics cause water to be retained within the proximal tubule and descending limb of loop of Henle (freely permeable to water)
Mannitol (Osmitrol) is an example of osmotic diuretic.
Clinical Use: mainly used to reduce increased intracranial pressure;
Osmotic diuretics: properties
mannitol (Osmitrol) : not metabolized, freely filtered at the glomerular
usually administered by IV; oral administration results in an osmotic diarrhea-- perhaps useful to promote elimination of toxic substances from the GI tract (in conjunction with activated charcoal)
urine volume increases with mannitol excretion due to direct osmotic effects
sodium reabsorption is reduced because of increased urine flow rates {decreased contact time between urine and tubular epithelial cells}
Clinical Uses:
To increase urine volume:
may be used to prevent anuria if the kidney due to hemolysis or rhabdomyolysis is presented with a large pigmented load.
when renal hemodynamics are compromised
To decrease intracranial or intraocular pressure:
Mannitol (Osmitrol) extract water from intracellular compartments, reducing total body water
Following IV administration, intracranial pressure falls within 60-90 minutes.
Toxicity:
Volume expansion effects -- increased extra cellular fluid volume and hyponatremia may cause pulmonary edema, complicating congestive heart failure
Headache, nausea, vomiting -- commonly observed
Dehydration and hypernatremia:
fluid loss leads to significant dehydration and in the absence of adequate fluid replacement leads to hypernatremia.
Ives, H.E., Diuretic Agents, in: Basic and Clinical Pharmacology, (Katzung, B. G., ed) Appleton-Lange, 1998, pp 242-259.
Diuretics: antihypertensive properties.
|
Distal Convoluted Tubule:From: Goodman and Gilman's "The Pharmacological Basis of Therapeutics, Ninth Edition
|
Acetazolamide (Diamox)
Glaucoma:
decreases rate of aqueous humor production -- leads to a declining in intraocular pressure
most common indication for use of carbonic anhydrase inhibitors
Dorzolamide (Trusopf): topical carbonic anhydrase inhibitor.
no diuretic or systemic metabolic effects
reduction in intraocular pressure comparable to oral agents
Urinary Alkalinization:
increased uric acid and cystine solubility by alkalinizing the urine (by increasing bicarbonate excretion)
for prophylaxis of uric acid renal stones, bicarbonate administration (baking soda) may be required
Metabolic Alkalosis:
Results from:
decreased total potassium with reduced vascular volume
high mineralocorticoid levels
These conditions are usually managed by treating the underlying causes; however, in certain clinical settings acetazolamide may assist in correcting alkalosis {e.g. alkalosis due to excessive diuresis in CHF patients}
Acute Mountain Sickness:
Symptoms: weakness, insomnia, headache, nausea, dizziness {rapid ascension of all of 3000 meters}; symptoms -- usually mild
In serious cases: life-threatening cerebral or pulmonary edema
Acetazolamide (Diamox) reduces the rate of CSF formation and decreases cerebral spinal fluid pH.
Prophylaxis against acute mountain sickness may be appropriate
Other Uses:
some role in management of epilepsy
hypokalemia periodic paralysis
increase urinary phosphate excretion during severe hyperphosphatemia.
Furosemide (Lasix), bumetanide (Bumex), torsemide (Demadex), ethacrynic acid (Edecrin)
Major Clinical uses:
acute pulmonary edema
acute hypercalcemia
management of edema
Other uses:
hyperkalemia:
loop diuretics increase potassium excretion
effect increased by concurrent administration of NaCl and water.
acute renal failure:
may increase rate of urine flow and increase potassium excretion.
may convert oligouric to non-oligouric failure {easier clinical management}
renal failure duration -- not affected
anion overload:
bromide, chloride, iodide: all reabsorbed by the thick ascending loop:
systemic toxicity may be reduced by decreasing reabsorption
concurrent administration of sodium chloride and fluid is required to prevent volume depletion
|
bendroflumethazide |
benzthiazide |
chlorothiazide (Diuril) |
chlorthalidone (Hygroton) |
|
hydrochlorothiazide (HCTZ, Esidrix, HydroDIURIL) |
hydroflumethiazide |
indapamide (Lozol) |
methyclothiazide |
|
metolazone (Zaroxolyn, Mykrox) |
polythiazide |
quinethazone |
trichlomethiazide |
Hypertension
Congestive heart failure
Nephrolithiasis (due to idiopathic hypercalciuria
Nephrogenic diabetes insipidus
Mannitol (Osmitrol)
To increase urine volume:
may be used to prevent anuria if the kidney due to hemolysis or rhabdomyolysis is presented with a large pigmented load.
when renal hemodynamics are compromised
To decrease intracranial or intraocular pressure:
Mannitol extract water from intracellular compartments, reducing total body water
Following IV administration, intracranial pressure falls within 60-90 minutes.
Amiloride (Midamor), triamterene (Dyrenium), spironolactone (Aldactone)
Reduction of potassium loss associated with thiazide or loop diuretic administration
Mineralocorticoid excess:
Conn's syndrome (primary hypersecretion)
ectopic ACTH production (primary hypersecretion)
secondary aldosteronism caused by:
congestive heart failure
hepatic cirrhosis
nephrotic syndrome
conditions that cause renal salt retention with reduced intravascular volume
other diuretics may further reduce intravascular volume thus worsening secondary aldosteronism
|
cardiac glycosides |
oral hypoglycemics |
aminoglycoside antibiotics |
|
uricosuric drugs |
non-steroidal anti-inflammatory drugs |
Adverse Diuretic effects and contraindications
Adverse Effects: Carbonic Anhydrase Inhibitors (Acetazolamide)
Toxicity:
hyperchloremic metabolic acidosis
due to reduction in body bicarbonate stores
renal stones:
bicarbonate loss is associated with:
phosphaturia
hypercalciuria (calcium salts, relatively insoluble at alkaline pH)
renal potassium loss:
increased sodium bicarbonate in the collecting tubule increases the lumen-negative and in inelectrical potential -- enhances potassium excretion
counteracted by potassium chloride administration
Others:
drowsiness, parathesias
accumulation in renal failure (CNS toxicity)
hypersensitivity reactions
Contraindications:
hepatic cirrhosis
urinary alkalinization will decrease ammonium ion trapping, increasing the likelihood of hepatic encephalopathy.
Adverse Effects: Loop Diuretics
Hypokalemia metabolic alkalosis:
increased delivery of NaCl and water to the collecting duct increases potassium and proton secretion-- causing a hypokalemic metabolic alkalosis
in managed by potassium replacement and by ensuring adequate fluid intake
dose-related hearing loss (in usually reversible)
more common:
with decreased renal function
with concurrent administration of other ototoxic drugs such as aminoglycosides
may cause gout
loop diuretics cause increased uric acid reabsorption in the proximal tubule, secondary to hypovolemic states.
Hypomagnesemia: loop diuretics cause:
reduction in sodium chloride reabsorption
decreases normal lumen-positive potential (secondary to potassium recycling)
Positive lumen potential: drives divalent cationic reabsorption (calcium magnesium)
Therefore, loop diuretics increase magnesium and calcium excretion.
hypomagnesemia may occur in some patients.
reversed by oral magnesium administration
furosemide: skin rash, eosinophilia, interstitial nephritis(less often)
Other toxicities:
Dehydration (may be severe)
hyponatremia (less common than with thiazides thought may occur in patients who increased water intake in response to a hypovolemic thirst)
Hypercalcemia may occur in severe dehydration and if a hypercalcemia condition {e.g. oat cell long carcinoma} is also present.
Adverse Effects: Thiazides
Toxicity:
Hypokalemic metabolic alkalosis and hyperuricemia
Impaired carbohydrate tolerance
may induce hyperglycemia
impaired pancreatic insulin release
decreased tissue glucose utilization
hyperglycemia may be partially reversed by correcting a hypokalemic state
Hyperlipidemia
5% to 15% increase in serum cholesterol and an increase in low-density lipoproteins.
Hyponatremia:
Significant adverse effect, occasionally life-threatening
Mechanism:
hypovolemia-induced increase in ADH
reduced renal diluting capacity
increased thirst
Prevention: decreasing the drug dose or limiting fluid intake
Allergic reactions:
Thiazides are sulfonamides: cross-reactivity within the group
photosensitivity {rare}
dermatitis {rare}
Extremely rare reactions:
hemolytic anemia
thrombocytopenia
acute necrotizing pancreatitis
Other reactions:
weakness
fatigue
paresthesias
Adverse Effects: Osmotic Diuretics
Toxicity:
Volume expansion effects -- increased extra cellular fluid volume and hyponatremia may cause:
pulmonary edema, complicating congestive heart failure
Headache, nausea, vomiting -- commonly observed
Dehydration and hypernatremia:
flow gloss leads to significant dehydration and in the absence of adequate fluid replacement leads to hypernatremia.
Adverse Effects: Potassium-Sparing Diuretics
Toxicity:
Hyperkalemia:
Potassium-sparing diuretics can cause significant hyperkalemia
Factors that increase the likelihood of hyperkalemia:
renal disease
presence of agents that reduce renin:
beta-blockers
nonsteroidal anti-inflammatory drugs (NSAIDs)
ACE inhibitors
angiotensin receptor blockers
hyperkalemia more likely when potassium-sparing diuretics are used as the only diuretic drug or in the presence of renal insufficiency.
Given in combination with thiazides, hypokalemia and metabolic alkalosis associated with thiazide use may be balanced by aldosterone antagonists
Since thiazide adverse effects may predominate {hyponatremia, metabolic alkalosis}, due to variations in bioavailability, individual dose adjustment of the two drugs may be better.
Hyperchloremic Metabolic Acidosis:
Acidosis cause by inhibition of proton secretion along with potassium secretion {similar to type IV renal tubular acidosis
Gynecomastia:
Endocrine abnormalities associated with synthetic steroids --spironolactone:
gynecomastia (breast enlargement)
impotence
benign prostatic hyperplasia
Acute Renal Failure:
triamterene (Dyrenium) plus indomethacin
Kidney Stones:
triamterene (Dyrenium) (poorly soluble) may precipitate in urine, causing renal stones:
Contraindications:
may cause severe (potentially fatal) hyperkalemia
potassium supplements should be discontinued prior to administration of aldosterone antagonists
patients with chronic renal insufficiency are at particular risk
hyperkalemia is also more likely to occur or it if beta-blockers or ACE inhibitors are concurrently administered
impairment of hepatic metabolism of triamterene spironolactone may require dose adjustment
Mechanisms whereby furosemide and thiazides are useful in calcium metabolism disorders management
Role of Diuretics in Calcium Metabolism
Loop Diuretics and Calcium Metabolism
Furosemide (Lasix)
Torsemide (Demadex)
Bumetanide (Bumex)
Inhibition of NaCl reabsorption in the thick ascending limb of the loop of Henle
inhibit the Na/K/2Cl transport system in the luminal membrane
reduction in sodium chloride reabsorption
decreases normal lumen-positive potential (secondary to potassium recycling)
Positive lumen potential: drives divalent cationic reabsorption (calcium magnesium)
Therefore, loop diuretics increase magnesium and calcium excretion.
hypomagnesemia may occur in some patients.
hypocalcemia does not usually develop because calcium is reabsorbed in the distal convoluted tubule.
{in circumstances that result in hypercalcemia, calcium excretion can be enhanced by administration of loop diuretics with saline infusion}
Thiazides and Calcium Metabolism
Mechanism of action:
Diuretic action:Inhibition of NaCl reabsorption from the distal convoluted tubule (luminal side)
enhanced calcium reabsorption in the distal convoluted tubule (unknown mechanism)
thiazides infrequently cause hypercalcemia but can unmask hypercalcemia due to other causes such as carcinoma, sarcoidosis, or hyperparathyroidism.
Thiazides: nephrogenic diabetes insipidus
Diabetes insipidus: impaired renal water conservation, caused by:
Inadequate vasopressin secretion (Central or cranial diabetes insipidus)
Insufficient kidney response to vasopressin (nephrogenic diabetes insipidus)
Induction of diabetes insipidus:
hypercalcemia
hypokalemia
postobstructive renal failure
lithium (incidence: as high as 33%)
demeclocycline (Declomycin)
Familial nephrogenic diabetes insipidus: X-linked, typically,recessive)
Thiazides are central in treatment of nephrogenic diabetes insipidus, reducing urine volume by up to 50%.
Other drugs:
Amiloride: by blocking lithium uptake by the sodium channel in the collecting duct, amiloride is the drug of choice for lithium-induced nephrogenic diabetes insipidus.
Mechanism of action:
Decrease in volume promotes increased proximal tubule reabsorption.
Decreased extracellular fluid volume results in compensatory mechanisms that increase NaCl reabsorption in the proximal tubule -- reducing the volume delivered to the distal tubule.
As a result, less free water is formed and polyuria is decreased
Since the effectiveness of thiazide diuretics in treating nephrogenic diabetes insipidus follows the extent of natriuresis, the effectiveness may be enhanced by decreasing sodium intake.
Jackson, E.K. Diuretics In, Goodman and Gillman's The Pharmacologial Basis of Therapeutics,(Hardman, J.G, Limbird, L.E, Molinoff, P.B., Ruddon, R.W, and Gilman, A.G.,eds) TheMcGraw-Hill Companies, Inc.,1996, pp. 685- 713
Jackson, E.K. Vasopressin and Other Agents Affecting the Renal Conservation of Water In, Goodman and Gillman's The Pharmacologial Basis of Therapeutics,(Hardman, J.G, Limbird, L.E, Molinoff, P.B., Ruddon, R.W, and Gilman, A.G.,eds) TheMcGraw-Hill Companies, Inc.,1996, pp.715-732
Chlorpropamide (Diabinese) and clofibrate (Abitrate, Atromid-S) : Central (Cranial) Diabetes Insipidus
Diabetes insipidus: impaired renal water conservation, caused by:
inadequate vasopressin secretion (Central or cranial diabetes insipidus)
inadequate kidney response to vasopressin (nephrogenic diabetes insipidus)
Clinical Presentations:
Large volumes of dilute (200 mOsm/kg) urine excreted
With normal thirst, polydipsia is present
By contrast with diabetes mellitus, the urine in diabetes insipidus is tasteless.
Central or cranial diabetes insipidus can be discriminated from nephrogenic diabetes insipidus by administration of desmopressin (DDAVP).
Urine osmolality will
increase following desmopressin administration in patients with central diabetes insipidus
have limited effect or no effect in patients with nephrogenic diabetes insipidus.
Causes of central diabetes insipidus:
Head injury (near the pituitary and/or hypothalamus
Hypothalamic or pituitary tumor
Cerebral aneurysms
CNS ischemia
CNS infections
Central diabetes insipidus: idiopathic or familial
familial: autosomal dominant (chromosome 20)
point mutations in the signal peptide and VP-neurophysin-- causing defects in synthesis, processing, and preprohoromone transport.
Treatment:
Primary treatment: (antidiuretic peptides): desmopressin (DDAVP)
Patients intolerant of desmopressin: chlorpropamide (Diabinese) (oral sulfonylurea)
Mechanism of action -- chlorpropramide
potentiates effects of residual, circulating vasopressin (reduces urine volume in more than 50% of patients)
Antidiuretic mechanisms of carbamazepine (Tegretol), clofibrate, chlorpropamide (Diabinese) have not been definitively determined.
If polyuria is insufficiently reduced by chlorpropramide, a thiazide diuretic may be added.
For short-term management, the combination of carbamazepine (Tegretol) and clofibrate (Abitrate, Atromid-S) will also decreased polyuria in central diabetes insipidus:
Serious, adverse effects associated with prolonged use of this combination are limiting
Jackson, E.K. Vasopressin and Other Agents Affecting the Renal Conservation of Water In, Goodman and Gillman's The Pharmacologial Basis of Therapeutics,(Hardman, J.G, Limbird, L.E, Molinoff, P.B., Ruddon, R.W, and Gilman, A.G.,eds) TheMcGraw-Hill Companies, Inc.,1996, pp.715-732.
Management of inappropriate secretion of antidiuretic hormone
Disease of impaired water excretion caused by inappropriate vasopressin secretion, resulting in:
hyponatremia
hypoosmolality
Clinical effects:
lethargy
muscle cramps
anorexia
coma
nausea
convulsions
vomiting
death
Clinical effects are seen only if excessive fluid intake (in oral or IV) occurs concurrently with inappropriate vasopressin secretion.
Causes:
malignancies
pulmonary disease
CNS injury/diseases
trauma
infections
tumors
surgery
drugs {cisplatin, Vinca alkaloids, cyclophosphamide (Cytoxan),chlorpropamide (Diabinese), thiazide diuretics, phenothiazines, carbamazepine (Tegretol), clofibrate, nicotine, narcotics, tricyclic antidepressants}
Treatment
water restriction
IV hypertonic saline
loop diuretics
drugs that reduce the ability of vasopressin to increase water permeability in the renal collecting ducts:demeclocycline (Declomycin)
Jackson, E.K. Vasopressin and Other Agents Affecting the Renal Conservation of Water In, Goodman and Gillman's The Pharmacologial Basis of Therapeutics,(Hardman, J.G, Limbird, L.E, Molinoff, P.B., Ruddon, R.W, and Gilman, A.G.,eds) TheMcGraw-Hill Companies, Inc.,1996, pp.715-732.
Mechanism by which lithium compounds may cause a syndrome like diabetes insipidus
Introduction
Vasopressin: regulates water conservation
Synonymous terms: vasopressin: arginine vasopressin (AVP): antidiuretic hormone (ADH)
Similar peptide: oxytocin-- common vasopressin and oxytocin receptor antagonists
binds to myoepithelial cells in the mammary gland (milk ejection) and on uterine smooth muscle cells (uterine contraction)
The antidiuretic system consists of:
CNS component (vasopressin synthesis, transport, storage, release)
supraoptic nucleus (SON)
paraventricular nucleus (PVN)
Renal collecting duct system
epithelial cells -- increased water permeability in response to vasopressin.
Increased plasma osmolality: increased vasopressin release
Factors affecting/modifying vasopressin release
hypovolemia
hypotension
hypoxia
drugs
pain
nausea
certain endogenous hormones
Regulation of vasopressin secretion
Osmotic Stimulation of Vasopressin Release
CNS structures: osmoreceptive complex
Osmosensitive: magnocellular neurons (SON, PVN)
Subfornical organ (SFO) project to SON/PVN
Organum vasculosum of the lamina terminalis (OVLT) project during clearing directly to SON/PVN
Hypovolemic/hypotension stimulation of Vasopressin Release:
Baroreceptors:
Blood volume (filling pressures)--baroreceptors in:
left atrium
left ventricle
pulmonary veins
Arterial blood pressure: baroreceptors -- carotid sinus and aorta
Nerve impulses from baroreceptors are carried:
by the vagus and glossopharyngeal nerves to the nucleus of the solitary tract
to the A1-noradrenergic cells in the caudal ventrolateral medulla
to the SON and PVN
Hormonal Effects
Vasopressin release: stimulation
acetylcholine (nicotinic)
glutamine
histamine (H1)
dopamine (D1 and D1)
neuropeptide Y
prostaglandins
aspartate
cholecystokinin
substance P
vasoactive intestinal peptide
angiotensin II
Vasopressin release: inhibition:
atrial natriuretic peptide
gamma aminobutyric acid (gaba)
opioids (dynorphin)
Drug Effects
Vasopressin Release: Stimulation
vincristine (Oncovin)
nicotine
morphine (high doses)
cyclophosphamide
tricyclic antidepressants
epinephrine
lithium (inhibits renal effects of vasopressin; enhances vasopressin release
Vasopressin Release: Inhibition
ethanol
glucocorticoids
haloperidol (Haldol)
promethazine (Pherergan)
phenytoin (Dilantin)
morphine (low dose)
fluphenazine (Prolixin)
oxilorphan
carbamazepine (Tegretol)(renal effects -- anti-diuresis; inhibits vasopressin secretion (central effect)
Inhibits antidiuretic effect of vasopressin
Lithium is used widely for management of bipolar disorder (manic- depressive).
Lithium uptake by the sodium channel in the collecting duct, causes lithium-induced nephrogenic diabetes insipidus.
Lithium polyuria: normally reversible
Mechanism of action:
reduces V2 receptor-mediated adenyl cyclase stimulation
Often, the antibiotic demeclocycline (Declomycin) reduces the antidiuretic effects of vasopressin (possibly because of reduced cyclic AMP)
Jackson, E.K. Vasopressin and Other Agents Affecting the Renal Conservation of Water In, Goodman and Gillman's The Pharmacologial Basis of Therapeutics,(Hardman, J.G, Limbird, L.E, Molinoff, P.B., Ruddon, R.W, and Gilman, A.G.,eds) TheMcGraw-Hill Companies, Inc.,1996, pp.715-732.
Thiazides
Hydrochlorothiazide (HCTZ, Esidrix, HydroDIURIL)
chlorthalidone (Hygroton)
Chlorothiazide (Diuril)
The thiazides act in the distal tubule to decrease sodium reabsorption (inhibits Na/Cl transporter).
As a result of decreased sodium and chloride reabsorption, a hyperosmolar diuresis ensues.
Delivery of more sodium to the distal tubule results in potassium loss by an exchange mechanism.
Thiazides also promote calcium reabsorption, in contrast to loop diuretics.
The initial decrease in blood volume followed by a longer-termed reduction in vascular resistance appears to account for the hypotensive effects of the thiazides.
Adverse Effects
Potassium depletion is a potentially serious side-effect that may require potassium supplementation and/or concurrent use of potassium-sparing diuretics.
Hyperuricemia may occur precipitating gout.
The increase in systemic uric acid is due to a decrease in the effectiveness of the organic acid secretory system.
Diabetic patient may have difficulty in maintaining proper blood sugar levels.
Indapamide (Lozol)
Metolazone (Zaroxolyn, Mykrox)
Potassium Sparing
Amiloride (Midamor)
Spironolactone (Aldactone)
Triamterene (Dyrenium)
Furosemide (Lasix), Bumetaninde (Bumex), Ethacrynic Acid (Edecrin)
Furosemide (Lasix),bumetanide (Bumex), and ethacrynic acid (Edecrin) are "high-ceiling" loop diuretics acting primarily at the ascending limb of the loop of Henle.
The effectiveness of these agents is related to their site of action because reabsorption of about 30 - 40% of the filtered sodium and chloride load occurs at the ascending loop.
Distal sites are not able to compensate completely for this magnitude of reduction of NaCl reabsorption.
Loop diuretics increase urinary Ca2+ in contrast to the action of thiazides.
Loop diuretics also increase renal blood flow by decreasing renal vascular resistance.
These drugs are rarely used in the management of hypertension because of their short duration of action and the availability of better drugs.
Adverse Effects
Ototoxicity
Furosemide (Lasix) and ethacrynic acid (Edecrin) block renal excretion of uric acid by competition with renal secretory and biliary secretory systems.
Therefore these agents can precipitate gout.
Potassium depletion.
Osmotic Diuretic: Mannitol (Osmitrol)
![]()
![]()
|
|