|
|
|
|
|
|
|
Medical Pharmacology Chapter 35 Antibacterial Drugs
|
|
|
|
|
|
|
Second Generation Cephalosporins: Cefuroxime
Clinical Cases
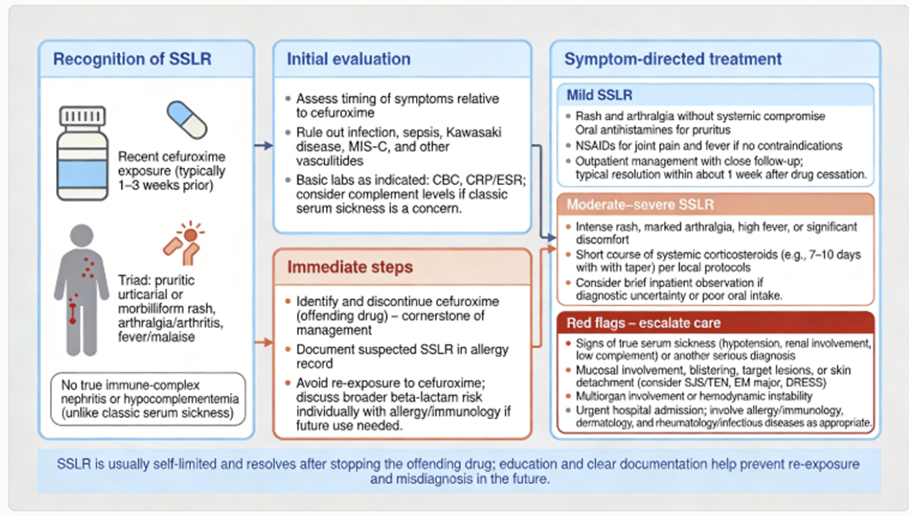
Case 1: Serum Sickness–Like Reaction to Cefuroxime – An uncommon immune-mediated adverse effect2
A 34-year-old woman was treated with cefuroxime for a post-partum breast infection (mastitis).
The infection improved, but about 7–10 days into therapy the patient developed a high fever, a widespread pruritic rash, and severe joint pains affecting her knees and ankles.
She had no shortness of breath or tongue swelling. Laboratory tests showed elevated inflammatory markers.
Clinically, this was consistent with a serum sickness–like reaction (SSLR).
Cefuroxime was immediately discontinued.
The patient was managed with corticosteroids and antihistamines, and her symptoms resolved over the next few days.
This case was reported in the literature: the authors noted that serum sickness–like syndrome, classically seen with cefaclor, can on rare occasions occur with other cephalosporins such as cefuroxime.2
In serum sickness-like reactions, patients develop immune complex deposition leading to rash, fever, and polyarthritis (but no true immune complex vasculitis as in classic serum sickness).
No permanent damage occurs if recognized and drug is stopped; the prognosis is good with supportive care.
This case shows that even a generally safe drug like cefuroxime can (very infrequently) cause significant immune-mediated reactions.
 |
Case 2: Cefuroxime-Induced Neurotoxicity in a Patient with Renal Failure (The importance of dose adjustment.)
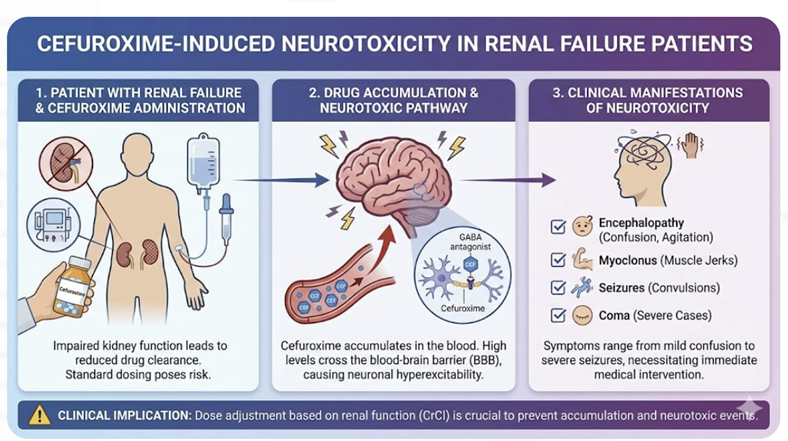 |
A 61-year-old woman with chronic kidney disease (baseline creatinine clearance ~20 mL/min) was admitted for a complicated urinary tract infection with possible pyelonephritis.3
Cultures grew Proteus mirabilis sensitive to cefuroxime, so she was started on high-dose IV cefuroxime 1.5 g every 8 hours.
Initially, the infection responded (fever improved).
However, after 9 days on cefuroxime, the patient became progressively lethargic and then unresponsive, with sporadic limb myoclonus (jerking movements) and horizontal nystagmus on exam.3
She had no history of seizures.
Laboratory workup showed her renal function had worsened (creatinine had risen, indicating acute-on-chronic renal failure).
Cephalosporin-induced neurotoxicity was suspected.
Cefuroxime was stopped immediately.
The patient was started on continuous venovenous hemodiafiltration (CVVH), a form of dialysis, in the ICU to remove the accumulated drug.3
Her plasma cefuroxime level at the start of dialysis was markedly elevated (~173 mg/L, whereas therapeutic peak levels are usually ~50–100 mg/L).
After 24 hours of dialysis, her cefuroxime level dropped to near-zero and her mental status completely normalized – she was awake, interactive, and had no neurological deficits.3
This case is a striking demonstration of β-lactam neurotoxicity.
Cephalosporins like cefuroxime, cefepime, and others are known to cause encephalopathy or seizures when not cleared (especially in the elderly or renally impaired patient).3 Here, the dose of cefuroxime had not be adjusted to account for the patient’s renal function, leading to accumulation.
The patient’s recovery after drug removal was complete, with no lasting effects.3
Always renally dose-adjust cefuroxime (and similar drugs), and monitor for neurological changes in high-risk patients.3
If unexplained encephalopathy occurs, both consider the antibiotic as potential responsible and take prompt action (e.g. stop the drug, provide supportive care, dialysis if needed).
With proper precautions, this situation is avoidable.
[This case was published as proof-of-concept that CVVH (a dialysis modality) is effective in clearing cefuroxime and treating cephalosporin neurotoxicity.]3
Case 3: Early Lyme Disease in Pregnancy – Cefuroxime as a Safe and Effective Therapy (Using cefuroxime when doxycycline is contraindicated.)
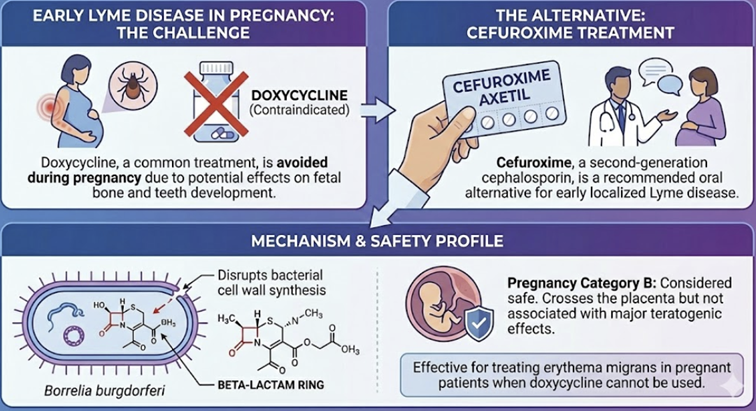 |
A 28-year-old pregnant woman in her second trimester presents in June with a classic erythema migrans rash (the “bull’s-eye” red rash) and flu-like symptoms.
The patient recalls a recent tick bite while hiking. Lyme disease is diagnosed clinically (and later confirmed by antibodies).
Doxycycline is the first-line treatment for early Lyme in most adults, but it is contraindicated in pregnancy (due to risks to the fetus’s developing bone and teeth).
The physician opts to treat with cefuroxime axetil, an alternative oral agent for Lyme.
The patient is started on cefuroxime 500 mg PO twice daily for 20 days.4
After 3–4 days of antibiotics, the patient experiences a mild Jarisch-Herxheimer reaction; she develops fever, chills, and an increase in the rash redness on day 1–2 of treatment, which resolves spontaneously by the next day.
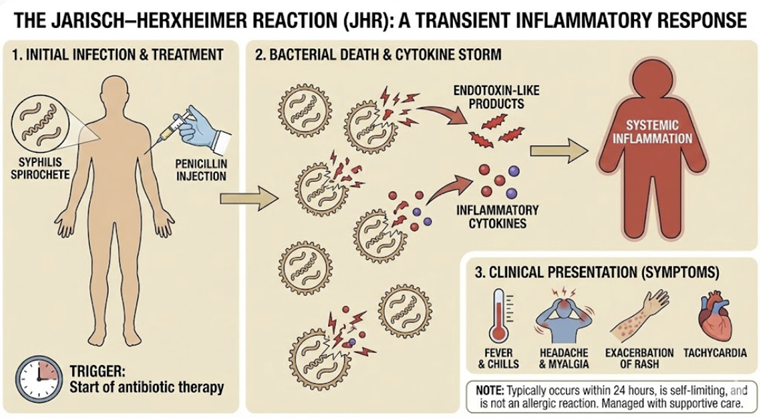 |
This transient reaction is due to endotoxin-like release from the dying spirochetes and is relatively common in Lyme therapy (occurring in about 5% of patients treated with cefuroxime for Lyme in trials).5
The patient is reassured and advised to rest, and the reaction abates.
The patient completes the 3-week course of cefuroxime.
Her rash and symptoms resolve completely, indicating successful cure of Lyme disease.
The patient continues her pregnancy without complications and later delivers a healthy baby.
This case highlights that cefuroxime is an excellent choice for Lyme disease during pregnancy, endorsed by guidelines as equally effective as doxycycline in early Lyme.4
This case also illustrates the Jarisch-Herxheimer phenomenon, which is not an allergic reaction but rather a sign of effective spirochete killing.
Understanding this aspect may prevent confusion between drug allergy vs. expected reaction.
Cefuroxime safety in pregnancy is well-established (no evidence of teratogenicity or fetal harm)4, making it a trusted treatment choice in this case.
Pediatricians use cefuroxime for Lyme in young children (<8 years old)
![]() Cefuroxime expands treatment
possibilities in populations where
tetracyclines are unsuitable, ensuring that
diseases like Lyme can still be treated
effectively and safely.
Cefuroxime expands treatment
possibilities in populations where
tetracyclines are unsuitable, ensuring that
diseases like Lyme can still be treated
effectively and safely.
Practice Questions and Answers
Question 1
A 60-year-old patient in the ICU develops hospital-acquired pneumonia. Sputum cultures grow a non-lactose fermenting, oxidase-positive Gram-negative rod identified as Pseudomonas aeruginosa. Which statement is TRUE regarding the use of cefuroxime in this situation?
A. Cefuroxime is a good choice, because it covers most Gram-negative rods including Pseudomonas.
B. Cefuroxime should be combined with an aminoglycoside to cover Pseudomonas.
C. Cefuroxime would not be effective, because Pseudomonas aeruginosa is resistant to cefuroxime.
D. Cefuroxime penetrates lung tissue poorly, so it cannot treat pneumonia.
Answer and Explanation: C is correct.
Pseudomonas aeruginosa is intrinsically resistant to cefuroxime and other second-generation cephalosporins.4
Cefuroxime has no activity against Pseudomonas, largely due to the bacterium’s efficient efflux pumps and restrictive outer membrane that prevent cefuroxime from reaching its targets, as well as Pseudomonas’ tendency to harbor potent β-lactamases.4
Therefore, cefuroxime would not be an appropriate treatment for a Pseudomonas pneumonia.
The correct approach would be to use an anti-pseudomonal antibiotic (such as ceftazidime, cefepime, piperacillin-tazobactam, a carbapenem like meropenem, or a fluoroquinolone active against Pseudomonas).
Options A and B are incorrect: Cefuroxime does not cover Pseudomonas at all, even in combination – combining it with another drug (B) doesn’t change that intrinsic lack of activity.
Option D is a false statement because cefuroxime does penetrate lung tissue well (it is indicated for pneumonia and achieves therapeutic levels in bronchial secretions).4
Cefuroxime should be avoided for this infection is not poor lung penetration, but rather the resistant organism.
In summary, cefuroxime should not be used for Pseudomonas infections. (Cefuroxime is suitable for many community-acquired pneumonias, but for hospital-acquired pneumonia with Pseudomonas, it is inappropriate.)
Question 2
A 30-year-old man with a severe penicillin allergy having experienced an anaphylactic reaction to penicillin in the past, has a methicillin-susceptible Staphylococcus aureus skin infection (cellulitis).
 |
|
The bacteria are sensitive to cefuroxime in vitro. What is the best course of action?
A. Use cefuroxime, since modern studies show negligible penicillin-cephalosporin cross-reactivity.
B. Avoid cefuroxime, and use a non-β-lactam alternative for MSSA (e.g. clindamycin or vancomycin).
C. Administer cefuroxime desensitization, then treat with cefuroxime.
D. Pretreat with an antihistamine and give cefuroxime under observation.
Answer and Explanation: B is correct.
In a patient with a documented anaphylactic reaction to penicillin, cefuroxime is contraindicated as a treatment choice.4
Although it is true that the cross-allergy between penicillins and second-generation cephalosporins like cefuroxime is much lower than once feared (option A references studies that found little to no cross-reactivity)5, standard medical practice is to err on the side of caution for severe IgE-mediated allergies.
Label and guidelines advise against using cephalosporins in patients with penicillin anaphylaxis, due to the risk (however small) of a life-threatening reaction.4
The safest and best approach is to choose a non-β-lactam antibiotic to treat the MSSA infection.
Clindamycin or vancomycin (depending on severity and MRSA risk) could be used for cellulitis in this penicillin-allergic patient.
Option C (desensitization) is generally not necessary for treating cellulitis because alternative antibiotics are available (desensitization is usually reserved for scenarios like syphilis in pregnancy where penicillin is absolutely required and no good substitutes exist).
Option D, giving antihistamines, would not prevent an anaphylactic reaction (it might mask mild allergy symptoms but would not stop an IgE-anaphylaxis).
The correct answer is to avoid cefuroxime entirely and use another class of antibiotic.
In summary, even though cefuroxime likely would not cross-react, it is contraindicated in penicillin-anaphylactic patients (patient safety first).
For less severe penicillin allergies, many cephalosporins can be used, but for true Type I hypersensitivity, perhaps they should be avoided.)
Question 3
A 25-year-old woman is treated with cefuroxime axetil for early Lyme disease after developing an erythema migrans rash. About 8–12 hours after her first few doses, she experiences fever, chills, muscle pains, and a transient worsening of her rash and symptoms.
What is the most likely explanation for this reaction?
A. An IgE-mediated allergic reaction to cefuroxime.
B. Antibiotic failure – the infection is getting worse, indicating resistance.
C. A Jarisch-Herxheimer reaction due to rapid killing of the spirochetes.
D. Superinfection with Clostridioides difficile (antibiotic-associated colitis).
Answer and Explanation: C is correct.
This clinical picture is classic for a Jarisch-Herxheimer reaction, which can occur during treatment of spirochetal infections like Lyme disease (as well as syphilis).5
The Jarisch-Herxheimer reaction is an acute, transient inflammatory response that happens when large numbers of bacteria are killed off quickly, releasing endotoxin-like substances.
In Lyme disease, patients may develop fever, chills, headache, and an increase in rash or other symptoms within the first day of antibiotic therapy.
The reaction is self-limiting, typically lasting a short time (hours to a day).
This reaction is not an allergic reaction.
Answer A is incorrect because an allergic reaction to cefuroxime would more likely produce hives, itching, bronchospasm or anaphylaxis rather than fever and generalized symptom flare.
Option B is incorrect since the infection is not truly “worsening” due to resistance (the symptoms are transient and due to dying organisms, not ongoing infection).
Jarisch-Herxheimer indicates that the antibiotic is working (killing the Borrelia spirochetes).
Option D (C. difficile colitis) would typically present with diarrhea and abdominal pain days to weeks later, not acute fever/chills on day 1 of therapy.
In clinical trials of Lyme treatment with cefuroxime, approximately 5.6% of patients experienced a Jarisch-Herxheimer reaction.5
Correct management is supportive care (anti-pyretics, fluids) while continuing antibiotic administration.
The reaction usually resolves on its own.
The patient’s reaction is best explained by the Jarisch-Herxheimer phenomenon.
As a counseling point for patients with Lyme disease: Patients should be warned about the possibility of a temporary symptom flare after starting treatment so they are not alarmed.
However, if a patient had trouble breathing or rash immediately after a dose, that would indicate an allergy, not seen in the case here.
Question 4
Which of the following infections is NOT appropriately treated by cefuroxime (cefuroxime as Ceftin tablets), assume the organism is susceptible and patient age is considered?
A. Acute otitis media in a 2-year-old child due to β-lactamase–producing H. influenzae.
B. Streptococcal pharyngitis (strep throat) in a 5-year-old child.
C. Early Lyme disease (erythema migrans) in a 15-year-old adolescent. (https://en.wikipedia.org/wiki/Erythema_migrans)
D. Community-acquired pneumonia due to penicillin-susceptible Streptococcus pneumoniae.
Answer and Explanation: B is correct
Cefuroxime tablets is not indicated for young pediatric strep throat.
While cefuroxime tablets is active against Streptococcus pyogenes, the FDA-approved indication for pharyngitis/tonsillitis is in patients ≥13 years old.
Cefuroxime tablets is not approved for treating strep throat in a 5-year-old; however Ceftin oral suspension is approved for treating mild-to-moderate pharyngitis/tonsillitis due to Streptococcus pyogenese.8
In practice, a 5-year-old with strep throat should receive penicillin or amoxicillin (first-line), or if allergic, perhaps azithromycin – but not cefuroxime tablets as a first choice.9 Choices A, C, and D are valid uses of cefuroxime.
For (A): Acute otitis media (AOM) in a toddler due to beta-lactamase–producing H. influenzae is a scenario where cefuroxime is appropriate.4
Cefuroxime is indicated for AOM and is effective against β-lactamase producing respiratory pathogens.
The oral suspension is commonly used in children for exactly this reason, especially if amoxicillin fails or the child has risk factors for resistant organisms.
For (C): Early Lyme disease in a 15-year-old can be treated with cefuroxime axetil. Lyme is an FDA-approved indication in patients ≥13, and a 15-year-old falls in that category.4
Cefuroxime is recommended by guidelines as an alternative to doxycycline for Lyme, so this is a correct use.
For (D): Community-acquired pneumonia (CAP) due to a penicillin-susceptible S. pneumoniae – cefuroxime (usually IV for inpatients, or oral for milder cases) is an accepted treatment.
IDSA guidelines include IV cefuroxime as one option for CAP, often combined with a macrolide for atypical coverage.4
Cefuroxime covers pneumococcus and H. influenzae, common CAP pathogens, so it is suitable.
February, 2026
|
|
|
|
|
|
|
|
|
This Web-based pharmacology and disease-based integrated teaching site is based on reference materials, that are believed reliable and consistent with standards accepted at the time of development. Possibility of human error and on-going research and development in medical sciences do not allow assurance that the information contained herein is in every respect accurate or complete. Users should confirm the information contained herein with other sources. This site should only be considered as a teaching aid for undergraduate and graduate biomedical education and is intended only as a teaching site. Information contained here should not be used for patient management and should not be used as a substitute for consultation with practicing medical professionals. Users of this website should check the product information sheet included in the package of any drug they plan to administer to be certain that the information contained in this site is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. Advertisements that appear on this site are not reviewed for content accuracy and it is the responsibility of users of this website to make individual assessments concerning this information. Medical or other information thus obtained should not be used as a substitute for consultation with practicing medical or scientific or other professionals. |