|
|
|
|
|
|
|
Medical Pharmacology Chapter 16: Pharmacology of Antipsychotics Drugs
|
|
|
|
|
|
|
Clinical Cases
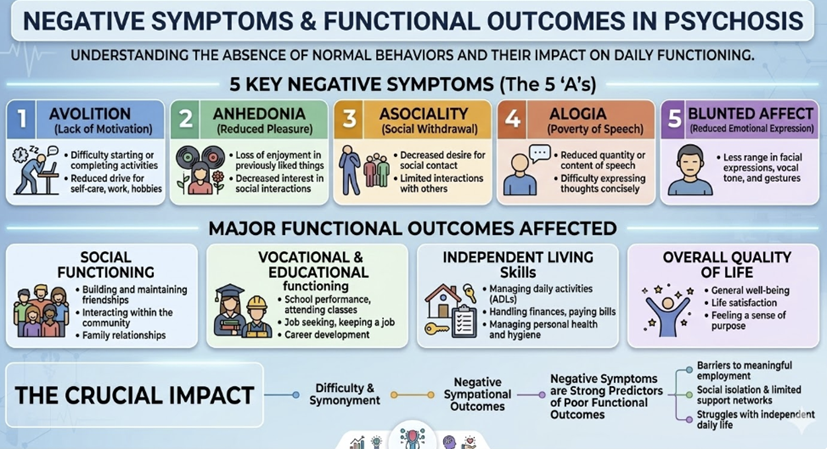
Case 4: Negative symptoms and functional outcome
A 24‑year‑old man with a first‑episode of schizophrenia 18 months ago has had good control of hallucinations and delusions on a low‑dose second‑generation antipsychotic.
He has not been hospitalized in the last year. However, he spends most of his time at home, rarely initiates conversation, and dropped out of college.
He says he “just doesn’t feel like doing anything” and “nothing seems fun.”
His mother reports he needs prompting for basic hygiene.
There is no clear depressed mood, guilt, or suicidal ideation.
Questions
What symptom domain is now most functionally impairing for him?
How would you clinically distinguish primary negative symptoms from depression and medication side effects?
Why are these symptoms so important for his long‑term prognosis, even though his positive symptoms are controlled?
What types of interventions (broad categories) could help address his deficits?
Explained answers
Most impairing domain
He exhibits prominent negative symptoms: avolition, anhedonia, alogia, and social withdrawal, with impaired role functioning and self‑care.
Positive symptoms are largely controlled, so functional impairment is being driven by this negative/cognitive domain.
Distinguishing negative symptoms from depression or side effects
Depression: look for pervasive sadness, guilt, hopelessness, marked diurnal variation, suicidal ideation where are not clearly present here.
In depression, patients often report distress about their low energy; in primary negative symptoms, there may be less subjective distress.
Medication side effects: evaluate for akinesia, extrapyramidal symptoms, sedation, or parkinsonism; use rating scales if needed and consider dose reduction or switching if EPS or sedation are prominent.
Primary negative symptoms persist despite optimized medication, minimal EPS, and absence of significant depressive features. Longitudinal observation helps: if these deficits preceded treatment and have remained relatively stable, they are more likely primary.
Prognostic importance
Negative and cognitive symptoms are among the strongest predictors of functional outcome (employment, independent living, social relationships) in schizophrenia and FEP.
Even with full positive symptom remission, persistent negative symptoms markedly reduce the likelihood of functional recovery, and they are harder to treat pharmacologically than positive symptoms.
Intervention types
Psychosocial:
Cognitive remediation and social skills training to improve cognitive and social functioning.
Behavioral activation and structured activity scheduling.
Supported employment/education (e.g., IPS) to scaffold return to roles.
Pharmacologic:
Optimize antipsychotic regimen to minimize sedation/EPS.
Consider agents with some evidence for negative symptoms in selected cases, though effects are modest.
Family involvement: psychoeducation so family supports realistic goals and avoids high expressed emotion, which can worsen motivation and engagement.
 |
|
|
|
|
|
|
|
DISCLAIMER
|