|
|
|
|
|
|
|
Medical Pharmacology Chapter 16: Pharmacology of Antipsychotics Drugs
|
|
|
|
|
|
|
|
 |
 |
 |
 |
|
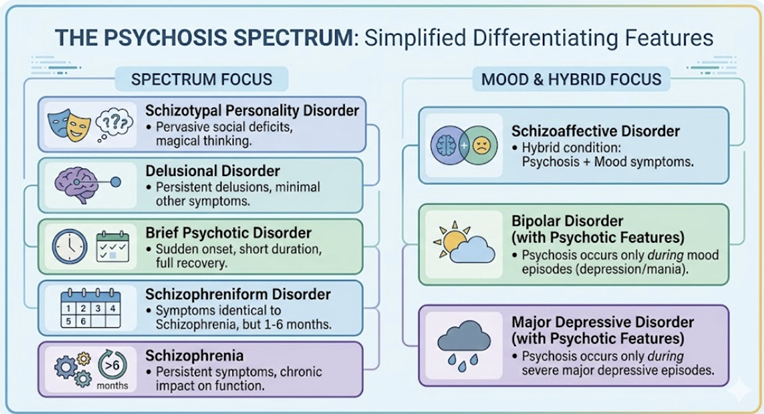
In terms of medical classification, psychosis is not a diagnosis in itself but rather a clinical syndrome, described by many signs and symptoms arising from a broad array of neurobiological, pharmacological, and systemic causes.
Psychosis represents a fundamental disruption in the individual's capacity to accurately perceive and interpret reality.1,4
Formal description is found in for example DSM-5-TR and the ICD-11, representing psychotic disorders along a dimensional spectrum.3,4
This classification reflects growing recognition that discrete categorical boundaries between psychotic disorders are not supported by neurobiology, genetics, or treatment response data.
![]() Schizophrenia,
schizoaffective disorder, schizotypal personality disorder, delusional
disorder, brief psychotic disorder, schizophreniform disorder, and the
psychotic features of bipolar disorder and major depressive disorder all
occupy positions along this spectrum, sharing overlapping
etiological, neurobiological, and phenomenological features.
Schizophrenia,
schizoaffective disorder, schizotypal personality disorder, delusional
disorder, brief psychotic disorder, schizophreniform disorder, and the
psychotic features of bipolar disorder and major depressive disorder all
occupy positions along this spectrum, sharing overlapping
etiological, neurobiological, and phenomenological features.
|
|
Historically, Eugen Bleuler introduced the term 'schizophrenia' in 1911, replacing Kraepelin's 'dementia praecox,' and identified the 'four As': affective blunting, associations (loosening of), autism (inward retreat), and ambivalence.
Kurt Schneider subsequently articulated his First Rank Symptoms consisting of phenomena considered pathognomonic of schizophrenia, including thought insertion, thought withdrawal, thought broadcasting, made feelings, made impulses, made volitional acts, somatic passivity, voices heard arguing or commenting in the third person, and delusional perception.3
While Schneiderian criteria have been deemphasized in the DSM-5 and ICD-11 in favor of polythetic, criteria-based diagnosis, these criteria remain conceptually instructive, serving as a framework for eliciting psychotic phenomena during the mental status examination.
![]() Clinical
manifestation of Psychosis
Clinical
manifestation of Psychosis
The clinical presentation of psychosis is extraordinarily rich and demands careful, thorough phenomenological assessment.
The traditional and enduringly useful approach organizes psychotic phenomena into three broad domains: positive symptoms, negative symptoms, and cognitive impairments.1,2
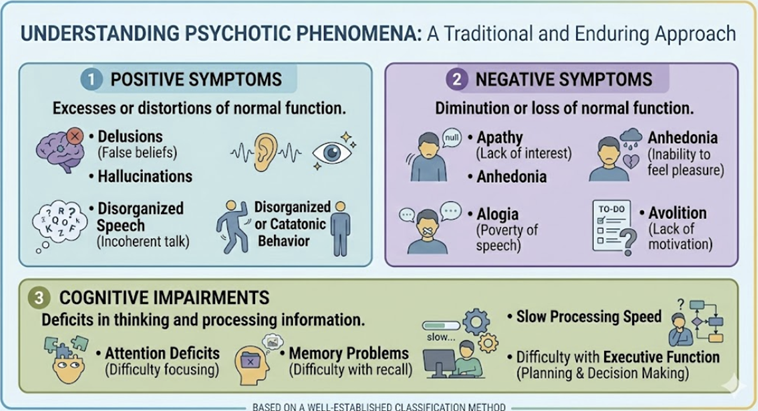 |
Contemporary investigators and clinicians have added mood and affective dysregulation as a fourth dimension and motor symptoms, including catatonia, as a fifth.
Understanding the interplay among these domains is essential not only for diagnosis but also for prognosis and treatment selection.
Hallucinations are perceptions that arise in the absence of an external stimulus, occurring with the quality of real perception in full consciousness , distinguishing them from illusions (misperceptions of real stimuli) and pseudohallucinations (perceptions experienced as coming from internal psychic space).1
Auditory hallucinations in schizophrenia most commonly take the form of voices usually typically experienced as external, fully formed, and distinct from the patient's own thoughts.
Content ranges widely:
Voices may comment on the patient's behavior (running commentary)
Issue commands of varying imperviousness
Converse with each other about the patient in the third person, or simply call the patient's name.4
Tactile, olfactory, and gustatory hallucinations should always prompt consideration of organic etiologies.
Formication (the sensation of insects crawling under the skin) is classically associated with stimulant intoxication and alcohol withdrawal.
Olfactory hallucinations are associated with temporal lobe epilepsy and mandate neurological evaluation.1
Visual hallucinations of elaborate, formed objects or scenes should raise organic suspicion
Visual hallucinations are more characteristic of delirium, dementia with Lewy bodies, Parkinson disease psychosis, and substance-induced states than of primary psychotic disorders.
Delusions are fixed, false beliefs held with extraordinary conviction, impervious to contrary evidence, and not accounted for by the individual's cultural, religious, or educational background.1,3
![]() Persecutory
delusions, beliefs that one is being harassed, followed,
surveilled, poisoned, or conspired against,are the single most
common form across all psychotic disorders.
Persecutory
delusions, beliefs that one is being harassed, followed,
surveilled, poisoned, or conspired against,are the single most
common form across all psychotic disorders.
Grandiose delusions are particularly characteristic of the manic phase of bipolar disorder.5,6
Delusions of reference involve the belief that neutral external events contain personalized messages directed at the patient.
Erotomanic delusions involve the conviction that another person is in love with the patient.
Disorganized Thought and Speech
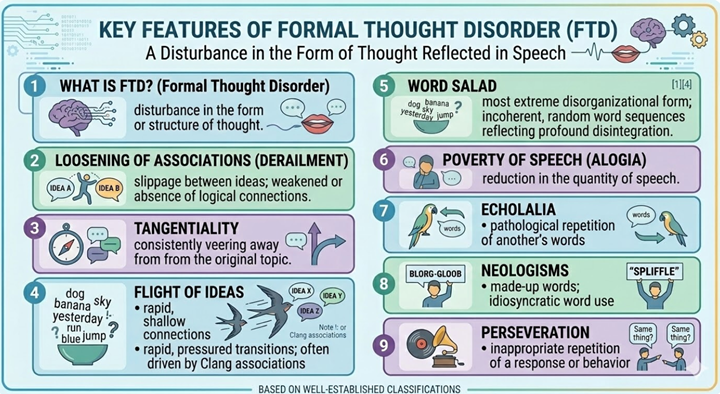 |
![]() Formal
thought disorder refers to a disturbance in the form or structure of
thought, reflected in the patient's speech.1,4
Formal
thought disorder refers to a disturbance in the form or structure of
thought, reflected in the patient's speech.1,4
Loosening of associations (derailment) refers to slippage between ideas where logical connections are weakened or absent.
Tangentiality occurs when the patient consistently veers away from the original topic.
Flight of ideas involves rapid, pressured transitions between loosely connected ideas, often driven by clang associations (a speech pattern where words are chosen based on sound (rhyming or alliteration) rather than meaning, resulting in illogical, incoherent, or nonsensical communication.).
Word salad.the most extreme disorganizational form. consists of incoherent, random word sequences reflecting profound disintegration of associative processes.
Poverty of speech (alogia), echolalia, neologisms, and perseveration are additional features the skilled clinician must recognize and document systematically.
Disorganized and Catatonic Behavior
Catatonia described in the DSM-5 as applicable to multiple conditions also presents along a continuum from the retarded/stuporous pole (mutism, immobility, negativism, posturing, catalepsy, waxy flexibility) to the excited pole (purposeless, excessive motor activity).18,19
The Bush-Francis Catatonia Rating Scale (BFCRS) (https://en.wikipedia.org/wiki/Catatonia) provides a validated assessment framework.
Catatonia is found in 5–18% of psychiatric inpatients yet remains underrecognized, carrying significant mortality risk when untreated, particularly if malignant catatonia or neuroleptic malignant syndrome develops.20,21
Benzodiazepines (lorazepam or diazepam) are first-line treatment.
ECT is reserved for refractory or malignant cases both are highly effective and must not be delayed.19
|
|
|
|
|
|
|
|
DISCLAIMER
|