"Narcotic" is a somewhat imprecise term
because it suggests "narcosis", which is indicated of a
somnolent state or "sleepy" state.
"Opioid analgesic" and
therefore is a more appropriate term emphasizing the
clinically important analgesic property which is the
pharmacological property of importance in the therapeutic
application of these agents.
Accordingly, opioids are used
without the expectation that they themselves will
cause sleep. However, opioids are frequently
used in combination with anesthetics and in that
context anesthesia may be obtained requiring less
anesthetic.
All natural/semisynthetic opium
alkaloid derivatives, synthetic agents, and
other agents whose opioid-like effects are
blocked by classical opioid antagonists, such as
naloxone (Narcan) or naltrexone (ReVia).
Opium -- from the opium
poppy (Papaver somniferum).
Opium is obtained
following drying the milky juice from unripe seed
pod.
Opium has a characteristic
odor and
bitter-taste with its chief active ingredient being
morphine. Also present are codeine, thebaine (a
non-analgesic agent), noscapine and papaverine, a
non-analgesic vasodilator.
Tincture of opium is
called laudanum.
Tincture is a generic term which refers
to an alcohol solution of a nonvolatile medicine. (Paregoric is a mixture of opium, alcohol, and camphor.)
An opioid full agonist
activates opioid receptors, exhibiting high
efficacy.
High efficacy refers to a maximal
opioid effect, typically pain relief.
Full
agonists may have comparable efficacies---the
differing potencies meaning that different amounts
of one drug compared to another may have to be
given in order to achieve a maximal effect.
A partial agonist may itself
cause agonist effects but because they can
displace through competitive action a full agonist
from its receptor, the net effect is a reduction
in drug effect. As a result, a partial
agonist, depending on circumstance, can act as
either in agonist or an antagonist.
Antagonists: Pharmacological
effects of opioids are mediated by interaction
with differing opioids receptor types.
Most
of the pharmacological effects as well as side
effects, at least respiratory depression, are
mediated by opioid-mu receptor interactions.
These agonist-mediated effects may be blocked by
competitive inhibition by agents that occupy the
the same receptor by do not activate it, yet
prevent activation by agonists.
Furthermore,
an opioid might be an agonist at one receptor
subtype, but only a partial agonist or even in
antagonist at another subtype.
Examples:
Naloxone
(Narcan):
pure antagonist: no
effects normally
associated with agonist
binding
Morphine:
full agonist at mu
receptor
Codeine:
partial or
"weak" agonist
-- less than maximal theoretical effect
despite complete receptor
saturation
Nalbuphine
(Nubain) : agonist at
one opioid receptor;
antagonist at another
Partial
agonist/antagonist
characteristics: replacement of
methyl moiety on the nitrogen
atom with larger substituents:
Allyl
substitution-- nalorphine and naloxone
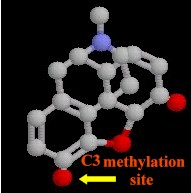
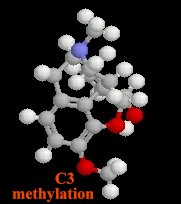
Substitutions
at the C3
and C6
morphine hydroxyl groups (see
below)
Pharmacokinetic
properties altered
Methyl
substitution at C3
reduces first-pass
hepatic metabolism by
glucuronide conjugation: -- as
a consequence codeine and
oxycodone have a higher
oral: parenteral potency
Morphine
Codeine and Oxycodone (methylated at C3)
Acetylation
of both morphine
hydroxyls = heroin (more
rapid access across the
blood-brain barrier
compared morphine); in
the brain heroin is rapidly
hydrolyzed to monoacetylmorphine and
morphine
Endogenous
Opioid Peptides: The rationale for
endogenous opioid peptides came from the idea that opioid
receptors are probably present in the body for the purpose of
interacting with endogenous or naturally occurring
substances. As a consequence, research proceeded to attempt
identification of these naturally occurring substances now known
as ß-endorphins and related peptides.
Morphine
(and related agents) cause analgesia by
acting at the brain regions containing
peptides which have opioid-like
properties
Previous used term
"endorphin" now refers to
ß-endorphins and related peptides
derived from the precursor: prepro-opiomelanocortin
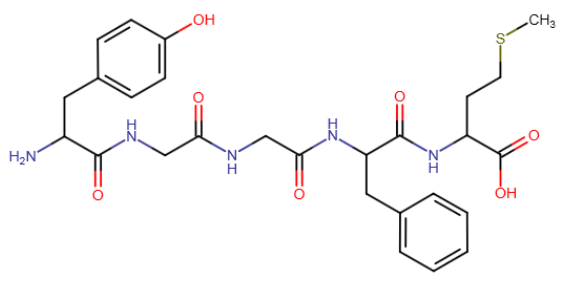
Most widely distributed
opioid analgesic peptides:
pentapeptides
Methionine-enkephalin
(met-enkephalin)
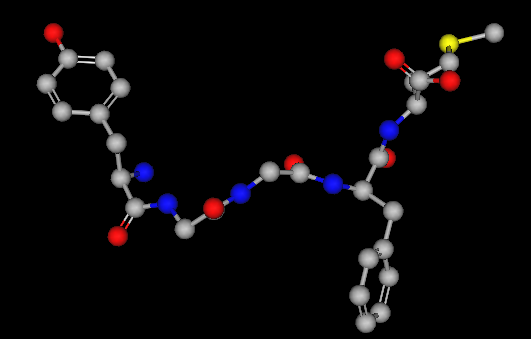
2D and 3D Met-Enkephalin Structure
Leucine-enkephalin
(leu-enkephalin)
Three major precursor
proteins:
Prepro-opiomelanocortin (POMC)
(contains):
Met-enkephalin
sequence
β-endorphin
sequence
some
nonopioid peptides:
ACTH
β-lipotropin
melanocyte-stimulating
hormone
Preproenkephalin
(proenkephalin A ) (contains):
six copies
of met-enkephalin
one copy
of leu-enkephalin
Preprodynorphin
(proenkephalin B) (contains--
active peptides containing the leu-enkephalin sequence):
dynorphin
A
dynorphin
B
α and β neoendorphin
Endogenous opioid precursors which are
localized at pain modulation brain
regions are probably released during stress, including
pain or pain anticipation.
Also, precursor molecules
for endogenous opioids are localized in adrenal medulla
and gut neural plexuses
Polar metabolites
-- renal; small amounts excreted
unchanged
Glucuronide conjugates --
bile (enterohepatic circulation minor)
Way, W.L.,
Fields, H.L. and Way, E. L. Opioid Analgesics and
Antagonists, in Basic and Clinical
Pharmacology, (Katzung, B. G., ed)
Appleton-Lange, 1998, pp 496-515.
Coda, B.A. Opioids, In
Clinical Anesthesia, 3rd Edition (Barash, P.G., Cullen, B.F. and
Stoelting, R.K.,eds)
Lippincott-Ravin Publishers, Philadelphia, New York,
1997, pp 329-358.
Schuckit, M.A.
and Segal D.S., Opioid Drug Abuse and Dependence, In
Harrison's Principles of Internal
Medicine 14th edition, (Isselbacher, K.J., Braunwald, E., Wilson, J.D., Martin,
J.B., Fauci, A.S. and Kasper, D.L., eds) McGraw-Hill, Inc
(Health Professions Division), 1998, pp 2508-2512.