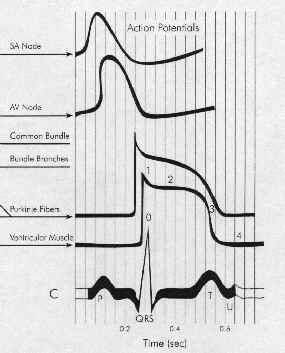
Five Phases: cardiac action potential associated with HIS-purkinje fibers or ventricular muscle
and ionic and electrophysiological
changes are associated with normal cardiac rhythm
Resting
membrane potential and conduction velocity
water-soluble, -- not free
to diffuse through the membrane in
response to concentration or electrical
gradients: depended upon membrane
channels (proteins)
Movement through channels
depend on controlling "molecular
gates"
Gate-status controlled by:
Ionic
conditions
Metabolic
conditions
Transmembrane
voltage
Maintenance
of ionic gradients:
Na+/K+
ATPase pump
termed
"electrogenic" when net
current flows as a result of
transport (e.g., three Na+
exchange for two K+
ions)
Initial
permeability state
-- resting membrane potential
sodium -- relatively
impermeable
potassium --
relatively permeable
Cardiac
cell permeability and conductance:
conductance: determined by
characteristics of ion channel
protein
current
flow = voltage X conductance
voltage =
(actual membrane potential -
membrane potential at which no
current would flow, even with
channels open)
Concentration gradient --
tends to drive potassium out
Electrical gradient tends to
hold K+
in.
Some K+
channels ("inward
rectifier") are open in the
resting state -- however, little K+ current flows because
of the balance between the K+ concentration and
membrane electrical gradients
In the resting membrane state, the m
gates are closed and the h gates are open: essentially
no Na+ flow.
Then with
depolarization, there is m gate activation
(activation gate); assuming
inactivation (h) gates are not
closed (when h gates are closed no sodium can
enter), then
Sodium
permeability dramatically
increased; intense sodium current
Depolarization
h gate closure; Na+
current inactivation
Ca2+
--
Ca2+: Channel
Activation Sequence similar to sodium; but occurring
at more positive membrane potentials (phases 1 and 2)
Following intense inward
Na+ current
(phase 0), Ca2+currents:
Phases 1 & 2, are slowly inactivated.
(Ca2+channel
activation occurred later than for Na+)
Channel
Inactivation, Re-establishing the Resting Membrane
Potential
Final repolarization
(phase 3):
complete Na+
and Ca2+ channel
inactivation
Increased potassium
permeability
Membrane potential
approaches K+
equilibrium potential -- which
approximates the normal resting membrane
potential
The extent and
synchrony of sodium channel activation is
dependent on the resting membrane potential.
Inactivation gates of sodium
channels close in the membrane potential
range of -75 to -55 mV (less channels
available for sodium ion inward current)
For example: less intense
sodium current if the resting potential
is - 60 mV compared to -80 mV
Consequences of
reduced sodium activation due to reduced
membrane potential (less negative)
reduced of
velocity upstroke (Vmax)
[phase 0] (maximum rate of
membrane potential change)
reduced
excitability
reduced
conduction velocity-- a
significant cause of arrhythmias
prolongation
of recovery:-- an increase in
effective refractory period
Plateau Phase:
Plateau phase -- Na
channels mostly inactivated
Repolarization (h gates
reopen)
"Refractory
period": time between phase 0 and phase 3 -- during this time the stimulus
does not result in a propagated response
Altered refractoriness may
cause or suppress arrhythmias
Factors that
reduce the membrane resting potential & reduce
conduction velocity
Hyperkalemia
Sodium pump block
Ischemic cell
damage
Conduction in
severely depolarized cells
With decreased membrane
potentials (e.g., -55 mV), sodium
channels are inactivated
Under some circumstances,
increased calcium permeability or
decreased potassium permeability allow
for slowly conducted action potentials
with slow upstroke velocity
Ca2+-inward
current-mediated action potentials are
normal for the specialized conducting SA
nodal and AV nodal tissues, which have
resting membrane potentials in the -50
to-70 mV range.
Hondeghem, L.M. and Roden, D.M.,
"Agents Used in Cardiac Arrhythmias", in Basic and Clinical
Pharmacology, Katzung, B.G., editor, Appleton & Lange, 1998, pp
216-241.
Factors
that may precipitate or exacerbate arrhythmias
Ischemia
Hypoxia
Acidosis
Alkalosis
Abnormal
electrolytes
Excessive
catecholamine levels
Autonomic
nervous system effects (e.g., excess
vagal tone)
Drug
effects: e.g., antiarrhythmic drugs may cause
arrhythmias)
Cardiac
fiber stretching (as may occur with
ventricular dilatation in congestive
heart failure)
Presence of scarred/diseased tissue which
have altered electrical conduction
properties
Hondeghem, L.M. and Roden, D.M.,
"Agents Used in Cardiac Arrhythmias", in Basic and Clinical
Pharmacology, Katzung, B.G., editor, Appleton & Lange, 1998, pp
216-241.
Factors that influence heart rate
(altered frequency of pacemaker cell firing rate)
Heart rate determined
(interval between pacemaker firing) by
the sum of: Action potential duration
+ Diastolic duration interval
More important -- Diastolic
duration interval: determined by 3
factors:
Maximum
diastolic potential (most
negative membrane potential
reached during diastole
Slope of
phase 4 depolarization:
(increased slope: threshold is
reached quicker causing a faster heart rate;
decreased slope: longer to reach
threshold resulting in a slower heart rate
Threshold
Potential (membrane potential at
which in action potential is
initiated)
Decreased Heart Rate:--
Vagal
Effects: (cholinergic
influences on the heart rate)
more negative
maximum diastolic potential (the
membrane potential starts farther
away from the threshold
potential)
reduced slope of
phase 4 depolarization (takes
longer to reach threshold
potential)
Increased Heart
Rate:-
Adrenergic
Effects: (sympathetic/sympathomimetic
influences on heart rate)
All cardiac cells (including
normally inactive atrial/ventricular
cells) may show pacemaker activity,
particularly in hypokalemic states
Failure of impulse
initiation can lead to excessively slow heart
rate,bradycardia .
If an impulse
fails to propagate through the conduction system
from the atrium to the ventricle, heart block may
occur.
An
excessively rapid heart rate, tachycardia,
is also encountered clinically
Hondeghem, L.M. and Roden, D.M.,
"Agents Used in Cardiac Arrhythmias", in Basic and Clinical
Pharmacology, Katzung, B.G., editor, Appleton & Lange, 1998, pp
216-241.