|
|
|
|
|
|
|
Medical Pharmacology Chapter 16: Pharmacology of Antipsychotics Drugs
|
|
|
|
|
|
|
Questions and Answers
How is psychosis diagnosed and what tools are used?
Overview1,2,3,4,5,6
Psychosis is diagnosed clinically, based on a careful history, examination, and longitudinal formulation, supported (but never replaced) by structured interviews, rating scales, and targeted medical workup.
The core tasks are:
(1) Confirming that psychotic symptoms are truly present
(2) Determining the underlying psychiatric or medical disorder, and
(3) Excluding secondary/organic and substance-induced causes.1,2,3,4,5,6
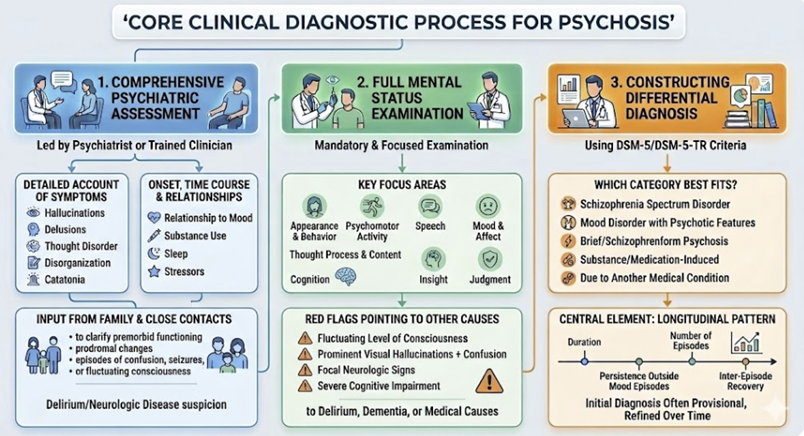
Core Clinical Diagnostic Process
Diagnosis begins with a comprehensive psychiatric assessment, usually led by a psychiatrist or similarly trained clinician.
This approach includes a detailed account of presenting symptoms e.g. hallucinations, delusions, thought disorder, disorganization, catatonia, their onset, time course, and relationship to mood, substance use, sleep, and stressors.
Related history from family or close contacts is strongly encouraged, particularly to clarify premorbid functioning, prodromal changes, and any episodes of confusion, seizures, or fluctuating consciousness that might suggest delirium or neurologic disease.1, 2,3,4
A full mental status examination is mandatory and focuses on appearance and behavior, psychomotor activity, speech, mood and affect, thought process and content (including systematic probing for delusions and abnormal perceptions), cognition (orientation, attention, memory, executive functions), insight, and judgment.
![]() Close
attention is paid to signs that point away from a primary
psychiatric disorder, such as fluctuating level of
consciousness, prominent visual hallucinations with
confusion, focal neurologic signs, or severe cognitive
impairment , which raise suspicion for delirium, dementia,
or other medical causes.1,5,6
Close
attention is paid to signs that point away from a primary
psychiatric disorder, such as fluctuating level of
consciousness, prominent visual hallucinations with
confusion, focal neurologic signs, or severe cognitive
impairment , which raise suspicion for delirium, dementia,
or other medical causes.1,5,6
At this stage, the psychiatrist also begins constructing a differential diagnosis using DSM-5/DSM-5-TR criteria, asking whether the presentation is best explained by a schizophrenia spectrum disorder, a mood disorder with psychotic features, a brief or schizophreniform psychosis, a substance/medication-induced psychotic disorder, or psychosis due to another medical condition.
The longitudinal pattern (duration of psychosis, persistence outside mood episodes, number of episodes, inter-episode recovery) is central, so diagnosis is often provisional initially and refined over time.1,4
 |
Screening and Specialized Clinical Interviews
First contact often occurs in primary care, emergency departments, or early psychosis services, where rapid screening for psychotic symptoms is essential.
Simple screening questions (e.g., asking about unusual experiences, hearing voices others do not hear, or strongly held odd beliefs) can flag patients for more detailed evaluation, and services such as CAMH provide examples of brief screening approaches.4,7
The “gold standard” for formal diagnosis uses structured or semi-structured diagnostic interviews that systematically map symptoms to DSM-5 criteria4,8,9
Structured Clinical Interview for DSM-5 (SCID-5): a comprehensive semi-structured interview used to establish or rule out major psychiatric diagnoses, including schizophrenia spectrum and mood disorders with psychotic features.4,8
Structured Interview for Psychosis-Risk Syndromes (SIPS) and related tools (e.g., Mini-SIPS): used in early psychosis clinics to characterize first-episode psychosis (FEP) and to identify individuals at clinical high risk (CHR-P) with attenuated psychotic symptoms.4,9
Other structured diagnostic interviews (e.g., Schedule for Affective Disorders and Schizophrenia) may be used in some research and specialty settings to refine diagnostic classification and differentiate psychotic from non-psychotic mood or anxiety conditions.4,10
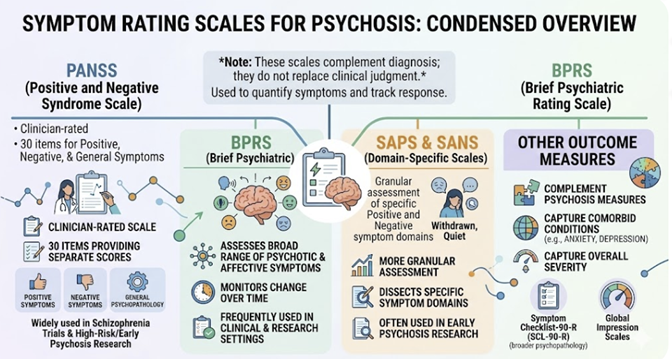
Symptom Rating Scales and Outcome Measures
Once psychosis is identified, standardized rating scales are used to quantify symptom severity and track treatment response, particularly in early psychosis and schizophrenia services.
These rating scales do not diagnose psychosis by themselves; they assume a clinical diagnosis has already been made.
Commonly used instruments include:
Positive and Negative Syndrome Scale (PANSS):
This 30‑item clinician-rated scale providing separate positive, negative, and general psychopathology scores.
This scale is widely used in schizophrenia trials and high-risk/early psychosis research.8,10
Brief Psychiatric Rating Scale (BPRS):
This scale assesses a broad range of psychotic and affective symptoms and is frequently used in both clinical and research settings to monitor change over time.10,11
Scale for the Assessment of Positive Symptoms (SAPS) and Scale for the Assessment of Negative Symptoms (SANS).
These tools are more granular in dissecting specific positive and negative symptom domains and are often used in early psychosis research.10
Other outcome scales (e.g., Symptom Checklist‑90‑R for broader psychopathology, global impression scales) complement psychosis-specific measures and help capture comorbid anxiety, depression, and overall severity.8
 |
|
|
|
|
|
|
|
|
DISCLAIMER
|