|
|
|
|
|
|
|
Medical Pharmacology Chapter 16: Pharmacology of Antipsychotics Drugs
|
|
|
|
|
|
|
Questions and Answers
![]() A
key step in diagnosing psychosis is systematically ruling out
general medical, neurologic, and substance-induced causes,
particularly in first-episode psychosis, atypical presentations, or
late-life onset.1,5
A
key step in diagnosing psychosis is systematically ruling out
general medical, neurologic, and substance-induced causes,
particularly in first-episode psychosis, atypical presentations, or
late-life onset.1,5
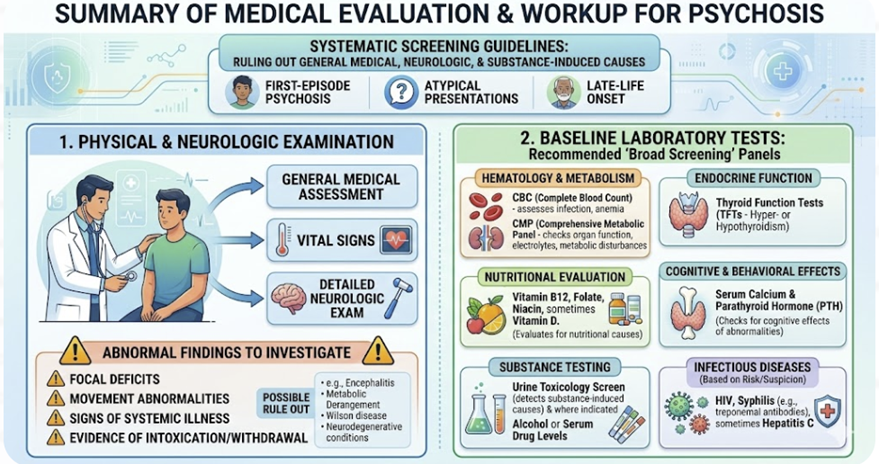 |
Guidelines and conceptual reviews converge on several elements:
(1) Physical and neurologic examination
![]() A
thorough physical exam, including vital signs, general
medical assessment, and detailed neurologic exam, is
recommended for all patients with new or unexplained
psychotic symptoms.
A
thorough physical exam, including vital signs, general
medical assessment, and detailed neurologic exam, is
recommended for all patients with new or unexplained
psychotic symptoms.
Abnormal findings, such as focal deficits, movement abnormalities, signs of systemic illness, or evidence of intoxication or withdrawal, strongly influence subsequent investigations and may point toward specific etiologies like encephalitis, metabolic derangement, Wilson disease, or neurodegenerative conditions.3,5,6,12
![]() Recommended
“broad screening” labs for first‑episode psychosis
commonly include:1,6,12
Recommended
“broad screening” labs for first‑episode psychosis
commonly include:1,6,12
Complete blood count and comprehensive metabolic panel (assess infection, anemia, organ function, electrolyte or metabolic disturbances).
Thyroid function tests (hyper- or hypothyroidism).
Vitamin B12, folate, niacin, and sometimes vitamin D, to evaluate for nutritional and metabolic causes of neuropsychiatric symptoms.1,3,12
Serum calcium and parathyroid hormone, given the cognitive and behavioral effects of calcium and parathyroid abnormalities.1,3
Urine toxicology screen and, where indicated, alcohol or other serum drug levels to detect substance-induced or interacting causes.3,5,12
Urine toxicology screen and, where indicated, alcohol or other serum drug levels to detect substance-induced or interacting causes.3,12
![]() Tests
for HIV, syphilis (e.g., treponemal antibodies), and
sometimes hepatitis C, based on epidemiologic risk and
clinical suspicion.12
Tests
for HIV, syphilis (e.g., treponemal antibodies), and
sometimes hepatitis C, based on epidemiologic risk and
clinical suspicion.12
(3) Neuroimaging and EEG1,5,13,14
Although not a universal requirement for routine brain imaging in every first‑episode psychosis, both literature reviews and more recent meta‑analyses assessments support obtaining CT or MRI at least once.
A clinically relevant abnormality is found in a nontrivial minority of patients, although brain imaging may be less useful in younger patients.
![]() Imaging
is strongly indicated when there are focal neurologic
signs, atypical features (e.g., sudden onset, rapidly
progressive deficits, seizures, severe headache), or
risk factors for structural brain disease.
Imaging
is strongly indicated when there are focal neurologic
signs, atypical features (e.g., sudden onset, rapidly
progressive deficits, seizures, severe headache), or
risk factors for structural brain disease.
EEG is considered when seizures, nonconvulsive status, or encephalopathy are suspected, especially in fluctuating or episodic presentations with prominent confusion or catatonia.
(4) Tiered and individualized approach
While there is no single, universally accepted “standard panel”, a reasonable assessment may involve a tiered approach beginning with broad screening and then proceeding to more targeted testing based on age, clinical features, and epidemiologic risk.
Main goals:
Identifying treatable secondary causes
Establish a medical baseline before initiating antipsychotics or mood stabilizers and
Avoid both under- and over-testing in vulnerable patients.5,6
|
|
|
|
|
|
|
|
DISCLAIMER
|