|
|
|
|
|
|
|
Medical Pharmacology Chapter 16: Pharmacology of Antipsychotics Drugs
|
|
|
|
|
|
|
Questions and Answers
What is the prognosis and recovery rates for psychosis?
Prognosis after a first episode of psychosis is heterogeneous but often substantially better than many patients and families fear, especially when there is early, sustained, and comprehensive treatment.
Outcomes differ by underlying diagnosis: bipolar disorder with psychotic features generally has higher long‑term recovery rates than schizophrenia spectrum disorders, and within schizophrenia the proportion achieving full recovery is modest but clinically meaningful.1,2,3,4,5,6
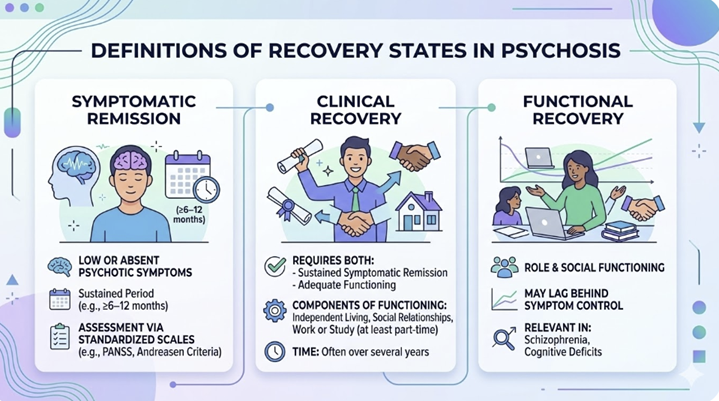
Defining prognosis: remission vs recovery
Prognostic estimates depend heavily on how “remission” and “recovery” are defined, which explains the wide range of numbers that have been reported in the medical literature.1,2,4,7
Symptomatic remission usually refers to low or absent psychotic symptoms for a sustained period (e.g., ≥6–12 months) with assessment often often based on standardized scales such as the PANSS and Andreasen criteria.1,2,4
Clinical recovery typically requires both sustained symptomatic remission and adequate functioning (e.g., independent living, social relationships, and at least part‑time work or study), sometimes over several years.1,4,6,7
Functional recovery alone (e.g., role and social functioning) may lag behind symptom control, which is particularly relevant in schizophrenia and in individuals with cognitive deficits.1,2,4,6
 |
Because stricter definitions (longer duration, higher functional thresholds, inclusion of affective and anxiety symptom remission) cut recovery rates substantially, any quoted percentage must be interpreted in light of its criteria and follow‑up period.1,4,6,7
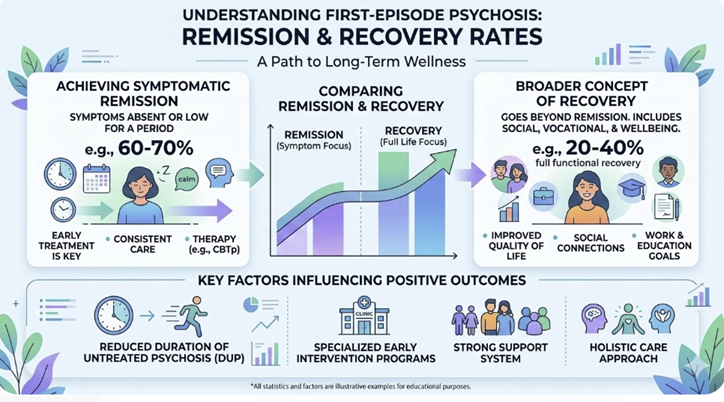
First‑episode psychosis: remission and recovery rates
A large systematic review of First Episode Psychosis (FEP) found that about 54% of patients were in symptomatic remission at a mean of 4 years after the first episode, and around 32% met criteria for recovery at a mean of 5.5 years.1
Another review reported mean remission rates around 58% over approximately 5.5 years, with recovery rates averaging about 38% over roughly 7.2 years, again across heterogeneous FEP samples.4
In an integrated early‑intervention program, symptom remission in FEP occurred in roughly 50% of individuals within the first 3 months, rising to approximately 75% by 6 months and over 80% by 1 year, although these figures reflect symptomatic improvement and not full functional recovery.2
A 10‑year follow‑up of FEP patients reported that about 59.9% achieved psychotic symptom remission for at least one year, 32.4% had adequate functioning, and 31.7% met a composite clinical recovery definition; applying a more stringent requirement of 5‑year remission roughly halved the recovery rates.7
Relapse remains common:
Three‑year follow‑ups in FEP cohorts suggest relapse rates of positive symptoms approaching 30–40% or more, especially when treatment is interrupted or adherence is poor.
Nonetheless, many patients experience an episodic course with substantial inter‑episode recovery rather than continuous psychosis.1,4,8
 |
Schizophrenia: long‑term outcome
When the underlying diagnosis is schizophrenia, long‑term prognosis is generally less favorable than for other psychotic disorders, but more contemporary medical research reports challenge the older view of uniformly chronic decline.4,6,9
A systematic review of schizophrenia outcomes in the 21st century estimated overall recovery rates between about 13% and 16%, depending on criteria, across contemporary treatment settings.6
For first‑episode schizophrenia specifically, five‑year clinical recovery rates (typically defined by remission plus reasonable functioning) have been estimated around 58% in some analyses, though these figures are sensitive to how schizophrenia is separated from other non‑affective psychoses and to loss to follow‑up.6,9,10
Across studies, remission rates in first‑episode schizophrenia over several years often range from roughly 36% to 60%, whereas full recovery (sustained remission plus good role and social functioning) is typically reported in the 17–30% range over longer follow‑up.1,4,6,10
![]() Schizophrenia
is not prognostically uniform: patients with prominent affective
symptoms, better premorbid adjustment, later onset, shorter duration of
untreated psychosis, and good early response to antipsychotics have
substantially better odds of functional recovery than those with
insidious onset, severe negative symptoms, and cognitive impairment.1,4,6,9
Schizophrenia
is not prognostically uniform: patients with prominent affective
symptoms, better premorbid adjustment, later onset, shorter duration of
untreated psychosis, and good early response to antipsychotics have
substantially better odds of functional recovery than those with
insidious onset, severe negative symptoms, and cognitive impairment.1,4,6,9
Bipolar disorder with psychosis: outcome compared with schizophrenia
In bipolar disorder, psychosis is associated with more severe acute episodes and more frequent hospitalization, but it does not consistently predict markedly poorer long‑term outcome compared with non‑psychotic bipolar disorder.5,11
A comprehensive review concluded that bipolar disorder with psychotic features is not invariably more severe than non‑psychotic bipolar disorder; some studies even linked absence of psychosis to more chronic affective courses and rapid cycling.11
In a 10‑year FEP cohort, patients whose primary diagnosis fell in the bipolar spectrum had higher clinical recovery rates (about 50%) than those with schizophrenia spectrum diagnoses (about 22.9%), despite similar social functioning metrics.7
In that analysis, individuals with schizophrenia proper showed the lowest clinical recovery rates (around 10.9%), while those with schizoaffective disorder and “other psychosis” had intermediate outcomes (roughly one‑third to 40% recovered), illustrating a gradient across diagnostic categories.7
Summary: these data support a general pattern in which bipolar psychosis tends to have better symptom and functional outcomes than schizophrenia, though mood‑incongruent psychotic features and persistent cognitive deficits can still portend more complex courses.5,7,11
![]() Predictors
of better vs poorer prognosis
Predictors
of better vs poorer prognosis
Predictors with better outcomes:
Across psychotic disorders, several factors repeatedly correlate with prognosis and recovery probabilities.1,2,4,8
Shorter duration of untreated psychosis (DUP), emphasizing the importance of early detection and rapid initiation of treatment.1,2,4,8
Good premorbid social and occupational functioning, higher educational attainment, and supportive family or social networks.1,4,6
Acute or subacute onset (as opposed to insidious deterioration), prominent affective symptoms, and relatively mild negative symptoms and cognitive impairment.1,4,6,9
Sustained engagement with early‑intervention or specialized psychosis services, adherence to evidence‑based pharmacotherapy, and access to psychosocial interventions (CBT for psychosis, family work, supported employment/education).2,4,6,12
![]() Factors associated with poorer prognosis or lower recover rates:
Factors associated with poorer prognosis or lower recover rates:
Diagnosis within the schizophrenia spectrum, especially schizophrenia, rather than bipolar or brief psychotic disorders.1,4,6,7
Early onset, male sex (in some cohorts), severe negative symptoms, prominent cognitive impairment, and substance use disorders.1,4,6,8,9
Long DUP (Duration of Untreated Pychosis), repeated relapses due to non‑adherence or inadequate treatment, and persistent social adversity such as unstable housing or unemployment.1,2,4,6,8
|
|
|
|
|
|
|
|
DISCLAIMER
|