|
|
|
|
|
|
|
-
What is the role of family support in FEP recovery?
-
Family support is one of the most powerful determinants of outcome in first‑episode psychosis (FEP), because most patients are young, live with relatives, and depend on family for day‑to‑day care, treatment adherence, and crisis management.
-
Supportive, low‑conflict families who receive structured psychoeducation and skills training can markedly reduce relapse, hospitalization, and symptom burden, whereas high criticism/hostility and chaotic environments (high expressed emotion) are consistently linked to poorer outcomes.1,2,3,4,5
-
-
How family support improves clinical and functional outcomes
-
Family involvement influences both symptom course and real‑world functioning in early psychosis.1,3,6,7
-
Relapse and rehospitalization:
-
Longitudinal work in early psychosis shows that stronger family support is associated with significantly fewer relapses, fewer hospital readmissions, and even lower mortality. Families that understand warning signs can prompt early help‑seeking, preventing full relapse.1,7
-
-
Treatment adherence:
-
Relatives often coordinate appointments, transport, medication refills, and communication with clinicians; when they are informed and engaged, adherence improves, which directly lowers relapse risk.1,6,7
-
-
Functional recovery:
-
Supportive families provide a stable base that facilitates return to school/work, social reintegration, and independent living skills, all of which are core components of “functional recovery” after FEP.1,2,3,8
-
-
Caregiver wellbeing and patient outcomes:
-
Interventions that reduce caregiver distress and improve coping (e.g., skills training, motivational interviewing–based programs) also improve family communication and create a more recovery‑conducive home environment.2,6,9
-
-
-
Families function as both co‑therapists and environmental “buffers,” amplifying the benefits of pharmacologic and psychosocial treatment.
-
-
Evidence for formal family interventions in FEP
-
 Family
interventions for psychosis (FIp), which usually combine
psychoeducation, communication skills, and problem‑solving, have
been tested specifically in FEP.1,10,11,12
Family
interventions for psychosis (FIp), which usually combine
psychoeducation, communication skills, and problem‑solving, have
been tested specifically in FEP.1,10,11,12
-
A Schizophrenia Bulletin meta‑analysis of FIp in FEP found that, compared with conventional care (with or without other psychosocial interventions), family intervention significantly reduced relapse risk up to 24 months (pooled risk ratio ≈0.42; conventional care alone RR ≈0.36).
-
FIp also reduced days hospitalized, lowered psychotic symptom severity, and substantially improved functioning (standardized mean difference >1 for functionality vs treatment as usual).10,11,13
-
-
A narrative and meta‑analytic review of family interventions in early psychosis concluded that FIp improves functioning and reduces relapse and carer distress, with symptom benefits that become more evident at follow‑up rather than immediately at end of treatment.1,12
-
Systematic reviews of family‑based early‑psychosis programs show benefits for both carers (reduced burden, better coping) and service users (better symptoms and functioning) compared with usual care.2,14
-
-
These findings
support including structured family work as a core component of
coordinated specialty care for FEP, not an optional adjunct.
-
-
Expressed emotion: risk and protective family processes
-
The quality of family involvement matters.1,3,5,7
-
High expressed emotion (EE), characterized by frequent criticism, hostility, or intrusive over‑involvement, is a well‑established risk factor for relapse in psychosis, including FEP. Families with high EE also report more burden and less adaptive coping.1,3,5
-
A recent systematic review of family functioning in FEP confirms that elevated EE (Expressed Emotion) is linked to worse clinical outcomes and higher relapse risk, whereas warm, open communication and supportive emotional expressiveness are associated with better symptom and relational outcomes.3
-
By contrast, “low‑EE” environments, calm, predictable, with warmth and non‑critical support, are associated with fewer relapses and better long‑term functioning; psychoeducation explicitly targets EE to shift families toward these patterns.1,3,7
-
*Psychoeducation is a structured, evidence-based therapeutic approach that teaches individuals and their families about mental health conditions, symptoms, and treatments.
-
This approach combines education with emotional support and skill-building to improve coping mechanisms, enhance treatment adherence, reduce stigma, and foster recovery.15,16,17
-
-
Summary: family support is protective when it takes the form of warmth and collaborative problem‑solving, but can become a risk factor when dominated by criticism, hostility, or unmodulated over‑involvement.
-
-
-
-
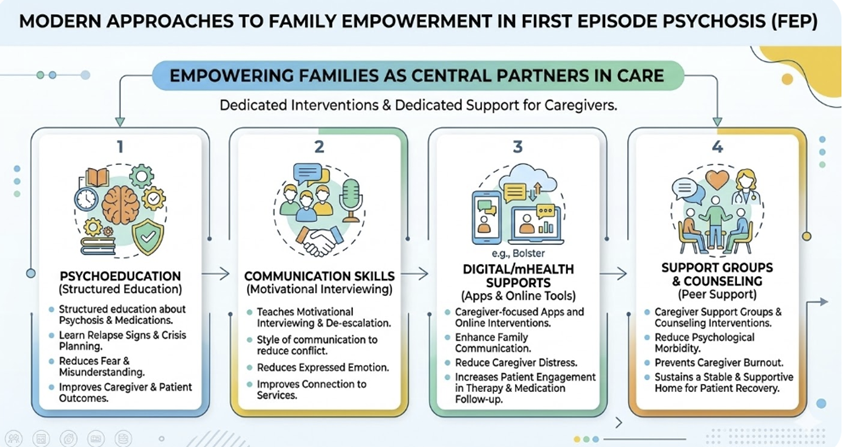
Modern approaches to empowering families
-
Current FEP programs increasingly view family members as central members of the treatment team and offer dedicated interventions to support them.2,4,6,8,9
-
Psychoeducation:
-
Structured education about psychosis, medications, relapse signs, and crisis planning, which reduces fear and misunderstanding and improves both caregiver and patient outcomes.1,2,8
-
-
Communication and motivational skills:
-
Programs teaching caregivers motivational interviewing, a style of communication and de‑escalation strategies that reduce conflict and expressed emotion. This approach can improve connection to services.6,9
-
-
Digital/mHealth supports:
-
New caregiver‑focused apps and online interventions (e.g., Bolster) appear promising in enhancing family communication, reducing caregiver distress, and increasing the likelihood that the young person engages in psychotherapy and medication follow‑up.2,9
-
-
Caregiver support groups and counseling: These interventions reduce caregiver psychological morbidity and burnout, which indirectly supports the patient’s recovery by sustaining a stable and supportive home.1,2,4,6
-
-
-
|
|
|
|
|
|
|