|
|
|
|
|
|
|
Medical Pharmacology Chapter 16: Pharmacology of Antipsychotics Drugs
|
|
|
|
|
|
|
Positive and Negative Symptoms
|
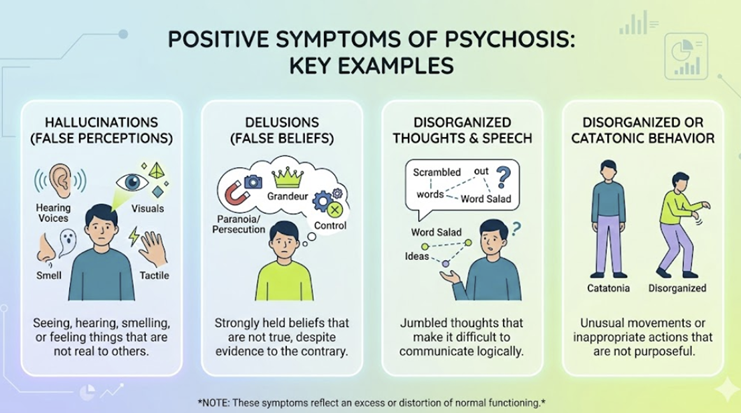
Positive symptoms represent phenomena added to normal experience or behavior and represent qualitative aberrations not normally present in healthy individuals.
Hallucinations26,27,28
Hallucinations are vivid, percept-like experiences occurring in the absence of an external stimulus, with a compelling sense of reality and not under voluntary control.
In psychotic disorders, auditory hallucinations predominate, frequently experienced as voices distinct from the patient’s own thoughts, often speaking in the third person, commenting on the patient’s actions, or conversing among themselves, features historically termed Schneiderian first-rank symptoms.
Visual hallucinations can occur but are less specific, and in the absence of substance use or neurological disease, complex, well-formed visual hallucinations should prompt careful evaluation for organic etiologies such as neurodegenerative disorders, epilepsy, or delirium.
Somatic, olfactory, and gustatory hallucinations are less common in primary psychotic disorders and more strongly suggest a neurological or medical substrate, especially temporal lobe or structural brain pathology, seizure disorders, or toxin exposure.
Delusions26,27,28
Delusions are fixed, false beliefs not amenable to change despite clear, conflicting evidence and not consistent with the person’s sociocultural background.
Common themes include persecutory delusions (belief that one is being harmed, monitored, or conspired against), grandiose delusions (exaggerated sense of power, knowledge, or identity), referential delusions (neutral events interpreted as having special personal meaning), erotomanic delusions (belief that another person, often of higher status, is in love with the patient), nihilistic delusions (belief that oneself or the world does not exist), and somatic delusions (false beliefs about bodily functions or structure).
Delusional systems may range from loosely organized, fragmentary ideas to elaborate, internally consistent constructs.
Clinicians should attend carefully to the degree of systematization, encapsulation, and whether delusional content is mood-congruent in affective psychoses.
Disorganized thinking and speech26,28 29,30
Disorganized thinking is inferred from disturbances in speech, reflecting disruption of the normal associative processes that link thoughts into coherent discourse.
Clinically, this appears as derailment or loose associations (ideas that shift from one topic to another with only tangential connection), tangentiality (answers obliquely related or unrelated to questions), circumstantiality (overinclusion of trivial or irrelevant details), or in more severe cases, incoherence or “word salad,” in which speech becomes nearly incomprehensible due to loss of logical and grammatical structure.
Neologisms (idiosyncratic creations of new words), clanging (associations based on sound rather than meaning), and perseveration are classic but less frequently encountered in modern clinical settings, and often herald more severe, chronic illness or acute decompensation.
Grossly disorganized or catatonic behavior26,28,30
Grossly disorganized behavior encompasses marked difficulties in organizing goal-directed behavior, from unpredictable agitation or silliness to bizarre or inappropriate dress, grooming, and social conduct.
Catatonia represents a syndrome of psychomotor disturbance and may include stupor, mutism, negativism, waxy flexibility, posturing, stereotypies, echolalia, and echopraxia, and while often associated with schizophrenia, it also occurs in mood disorders, neurodevelopmental disorders, and general medical conditions.
![]() Positive
symptoms are not specific to schizophrenia but represent a common
element of psychosis across all conditions.
Positive
symptoms are not specific to schizophrenia but represent a common
element of psychosis across all conditions.
 |
|
Positive symptoms represent phenomena added to normal experience or behavior that is qualitative aberrations not normally present in healthy individuals.
Positive Symptoms are not specific to schizophrenia but represent the common currency of psychosis across all conditions
The dopamine hypothesis attributes positive symptoms primarily to dopaminergic hyperactivity in the mesolimbic pathway, projecting from the ventral tegmental area (VTA) to limbic structures including the nucleus accumbens, amygdala, and hippocampus.11,12
Converging evidence supports this as virtually all effective antipsychotic agents block D2 receptors.
Furthermore, dopaminergic agents such as amphetamine can induce or worsen positive symptoms.
PET imaging demonstrates elevated striatal dopamine synthesis capacity in schizophrenia compared to controls.13,22
A revised dopamine hypothesis suggests that mesolimbic hyperdopamineric activity drives positive symptoms while mesocortical reduced dopamine activity underlies negative and cognitive symptoms.12,14
The salience dysregulation model proposes that aberrant dopamine firing attributes pathological 'incentive salience' to irrelevant stimuli, generating the sense of heightened significance that underpins delusion formation.14
This model elegantly integrates genetic predisposition, environmental stress, and the phenomenology of early psychosis.
The FDA approval of xanomeline-trospium (Cobenfy) in September 2024, the first exclusively muscarinic-cholinergic antipsychotic represents a paradigm-shifting development, demonstrating that non-dopaminergic mechanisms can effectively address psychosis.3
Negative Symptoms
Negative symptoms represent deficits in normal functioning and are among the most clinically challenging aspects of schizophrenia because they are less responsive to available treatments, are powerful predictors of functional impairment, and are frequently misidentified, attributed to depression, antipsychotic-induced akinesia, or demoralization.2
Careful disentanglement of 'primary' negative symptoms (intrinsic to the illness) from 'secondary' negative symptoms (caused by positive symptoms, depression, or medication side effects) is essential.
![]() The five
canonical negative symptoms organize into two higher-order factors. 'Diminished
expression' encompasses affective blunting (reduced facial expressions,
eye contact, vocal prosody, and expressive gestures) and alogia
(poverty of speech). 'Avolition-apathy' encompasses avolition
(reduced goal-directed initiation), anhedonia (diminished
anticipatory and consummatory pleasure), and asociality — the
collectively termed 'five As.2
The five
canonical negative symptoms organize into two higher-order factors. 'Diminished
expression' encompasses affective blunting (reduced facial expressions,
eye contact, vocal prosody, and expressive gestures) and alogia
(poverty of speech). 'Avolition-apathy' encompasses avolition
(reduced goal-directed initiation), anhedonia (diminished
anticipatory and consummatory pleasure), and asociality — the
collectively termed 'five As.2
Longitudinal research demonstrates that 73% of patients with negative symptoms experienced them before the onset of positive symptoms.2
The Brief Negative Symptom Scale (BNSS) and Clinical Assessment Interview for Negative Symptoms (CAINS) provide greater measurement precision than older instruments.
![]() The
neurobiological substrate of negative symptoms is distinct from positive
symptoms.
The
neurobiological substrate of negative symptoms is distinct from positive
symptoms.
Glutamatergic dysfunction at NMDA receptors is strongly implicated: ketamine and PCP, both NMDA receptor antagonists, produce a syndrome resembling schizophrenia in healthy volunteers that includes both positive and negative symptoms.
This is a phenomenon the dopamine hypothesis alone cannot account for.4,13
NMDA receptor hypofunction is a leading target for novel therapeutics addressing negative and cognitive symptoms
|
Cognitive Impairment26,28,31
Cognitive impairment is increasingly regarded as a core dimension of psychosis, particularly in schizophrenia, affecting attention, working memory, executive function, and social cognition.
![]() These
deficits often precede the onset of frank psychosis, remain relatively
stable over the course of illness, and strongly influence functional
outcomes, including employment and independent living.
These
deficits often precede the onset of frank psychosis, remain relatively
stable over the course of illness, and strongly influence functional
outcomes, including employment and independent living.
Affective symptoms26,28,33,34
Affective symptoms such as depression, anxiety, irritability, and dysphoria are highly prevalent across psychotic disorders, sometimes dominating the clinical picture and complicating differential diagnosis with primary mood disorders.
![]() Suicidality is a major concern, particularly in early psychosis and
post-psychotic depression, and requires active, ongoing assessment; a
substantial proportion of individuals with schizophrenia or bipolar disorder
with psychotic features attempt suicide at some point in their illness.
Suicidality is a major concern, particularly in early psychosis and
post-psychotic depression, and requires active, ongoing assessment; a
substantial proportion of individuals with schizophrenia or bipolar disorder
with psychotic features attempt suicide at some point in their illness.
|
|
|
|
|
|
|
|
DISCLAIMER
|