|
|
|
|
|
|
|
Medical Pharmacology Chapter 16: Pharmacology of Antipsychotics Drugs
|
|
|
|
|
|
|
Schizophrenia: Syndrome Overview and Diagnostic Criteria
![]() Schizophrenia
affects approximately 1% of the global population, with a lifetime
prevalence of approximately 0.4% in well-designed epidemiological
studies, accounting for a disproportionate share of a global psychiatric
disability that ranks among the top 10 global causes of disability.1,4
Schizophrenia
affects approximately 1% of the global population, with a lifetime
prevalence of approximately 0.4% in well-designed epidemiological
studies, accounting for a disproportionate share of a global psychiatric
disability that ranks among the top 10 global causes of disability.1,4
Schizophrenia typically manifests in late adolescence or early adulthood, with peak incidence in males in the early-to-mid twenties and in females in the late twenties.
A secondary peak in female onset occurs around menopause, consistent with the proposed neuroprotective role of estrogen in modulating dopaminergic transmission.4
![]() Schizophrenia is associated with substantially elevated mortality as
described by a shortening life expectancy by an estimated 13–15 years.
Schizophrenia is associated with substantially elevated mortality as
described by a shortening life expectancy by an estimated 13–15 years.
This decline in lifespan occurs due to cardiovascular disease, metabolic syndrome, smoking, and suicide.1
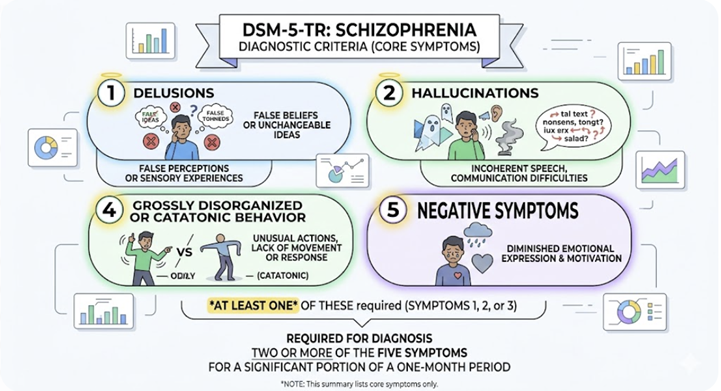 |
![]() The
DSM-5-TR diagnostic criteria require
two or more of the following five symptom criteria for a significant
portion of a one-month period:
The
DSM-5-TR diagnostic criteria require
two or more of the following five symptom criteria for a significant
portion of a one-month period:
(1) delusions,
(2) hallucinations
(3) disorganized speech
(4) grossly disorganized or catatonic behavior, and
(5) negative symptoms, with at least one of the first three required.1
Continuous signs of disturbance must persist for at least six months, and significant functional impairment must be evident.
Systematic medical workup before confirming a primary psychotic disorder is mandatory, including urine toxicology, CBC, comprehensive metabolic panel, thyroid function, HIV, syphilis serology, and brain imaging where clinically indicated.
The Prodromal Phase
Up to 75% of individuals with schizophrenia experience a recognizable prodromal phase lasting months to several years before transition to overt psychosis.4
Prodromal features include attenuated positive symptoms, cognitive decline, social withdrawal, declining academic and occupational performance, deteriorating self-care, dysphoria, anxiety, and sleep disturbances.
Negative symptoms often predominate, creating diagnostic difficulty because these nonspecific features can mimic depression or emerging personality pathology.
The concept of Clinical High Risk (CHR) for psychosis includes a at-risk mental state (ARMS) or ultra-high risk (UHR) and has been a focus of research.3,24
![]() The annual
rate of transition from CHR to full psychosis is approximately
22–35% over two years in clinical samples, and early
intervention represents one of the most promising frontiers in
preventing the long-term disability of schizophrenia.
The annual
rate of transition from CHR to full psychosis is approximately
22–35% over two years in clinical samples, and early
intervention represents one of the most promising frontiers in
preventing the long-term disability of schizophrenia.
Schizophrenia Spectrum Disorder Subtypes
The DSM-5 eliminated the traditional clinical subtypes of schizophrenia i.e. paranoid, disorganized, catatonic, undifferentiated, and residual, based on evidence that the approach lacked temporal stability, showed poor inter-rater reliability, and failed to predict differential treatment response.3
The DSM-5 adopted a dimensional approach assessing eight symptom domains on a 0–4 scale.
Despite their formal removal, these subtypes describe recognizable clinical phenotypes, and the ICD-11 retains some distinctions.
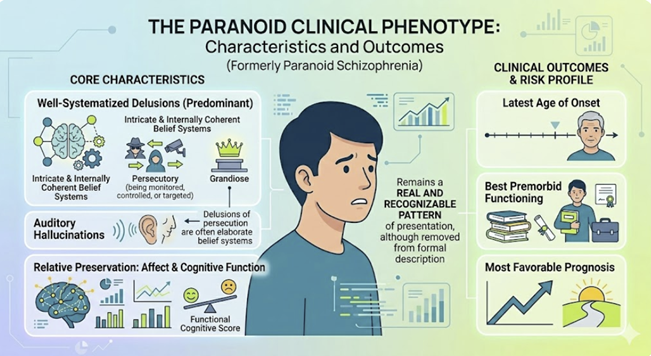 |
Paranoid schizophrenia was characterized by the predominance of well-systematized delusions, most commonly persecutory and/or grandiose along with auditory hallucinations, with relative preservation of affect and cognitive function.1,3
This subtype had the latest age of onset, best premorbid functioning, and most favorable prognosis.
The characteristics of persecutory delusions, sometimes intricate, have been described as an elaborate, internally coherent belief systems about being monitored, controlled, or targeted.
Paranoid clinical phenotype, although removed from formal description, remains a real and recognizable pattern of presentation.
Disorganized Schizophrenia (Hebephrenia) (obsolete term for a schizophrenia subtype, https://en.wikipedia.org/wiki/Disorganized_schizophrenia )
Disorganized schizophrenia (hebephreniaup to ICD10) was defined by disorganized speech, disorganized behavior, and flat or inappropriately silly affect.4
This subtype had the earliest onset, most insidious course, most severe cognitive impairment, and poorest prognosis.
Delusions and hallucinations tended to be fragmentary rather than systematized.
The characteristic inappropriate giggling, grimacing, and and unpredictable behavior required differentiation from organic conditions, particularly frontal lobe pathology.
Catatonic schizophrenia has become substantially rarer in the antipsychotic era but still should be promptly identified clinically.18,19
Catatonic schizophrenia now appears most frequently in mood disorders notably in bipolar disorder and severe depression, autoimmune encephalitides particularly inly anti-NMDA receptor encephalitis (https://en.wikipedia.org/wiki/Anti-NMDA_receptor_encephalitis), and metabolic derangements.
DSM-5 reformulated this type of catatonia as a cross-diagnostic specifier requiring three or more of twelve criteria.20
|
|
|
|
|
|
|
|
DISCLAIMER
|