|
|
|
|
|
|
|
Medical Pharmacology Chapter 16: Pharmacology of Antipsychotics Drugs
|
|
|
|
|
|
|
The intersection of psychosis and bipolar disorder (BD) represents one of the most diagnostically complex areas in psychiatry.
Psychotic symptoms both delusions or hallucinations fundamentally alter the illness phenotype, its clinical correlates, its prognosis, and its treatment.5
Understanding psychosis within bipolar disorder is essential for accurate diagnosis and optimal care.
Systematic reviews and meta-analyses strongly suggest that psychotic symptoms occur in approximately 50–75% of individuals with Bipolar I Disorder over the lifetime of the illness, primarily during manic episodes.5,23
In Bipolar II Disorder, psychosis is by definition absent during hypomanic episodes, but psychotic features during major depressive episodes may occur and are often underdetected.
Psychotic BD does not appear consistently associated with a distinct sociodemographic profile, suggesting psychotic features may represent an episode-level modifier rather than a stable trait marker.5
Mood-Congruent vs Mood-Incongruent Psychosis (Mood congruence: https://en.wikipedia.org/wiki/Mood_congruence)
Psychotic symptoms in bipolar disorder are classified as mood-congruent or mood-incongruent, a distinction with diagnostic, pathophysiological, and prognostic implications.5,25
Mood-congruent psychotic features are consistent with the prevailing mood state: during mania, grandiose delusions and affirmatory hallucinations; during depression, delusions of guilt, worthlessness, nihilistic or Cotard-type delusions (Cotard's Syndrome: https://en.wikipedia.org/wiki/Cotard's_syndrome), and self-punitive hallucinations.
Mood-incongruent features do not align with the prevailing mood state, and their presence has been associated with greater illness severity, longer episodes, and poorer functional outcomes.25
![]() Differential
Diagnosis: Bipolar I versus Schizophrenia versus Schizoaffective
Disorder
Differential
Diagnosis: Bipolar I versus Schizophrenia versus Schizoaffective
Disorder
The differentiation of psychotic bipolar disorder from schizophrenia and schizoaffective disorder is a diagnostic challenge.5,6
Rapid psychomotor activation, decreased sleep without fatigue, pressured speech, grandiosity, pronounced mood elevation, and a cyclical episodic course with full interepisodic recovery suggest bipolar disorder.
Prominent, sustained negative symptoms, formal thought disorder, and impaired premorbid functioning (Below-average cognitive, social, or academic performance existing prior to onset of the major psychiatric disorder) unrelated to mood state suggest schizophrenia.
The temporal relationship between psychosis and mood symptoms is the key axis of longitudinal differentiation.24
Sustained longitudinal observation is required.
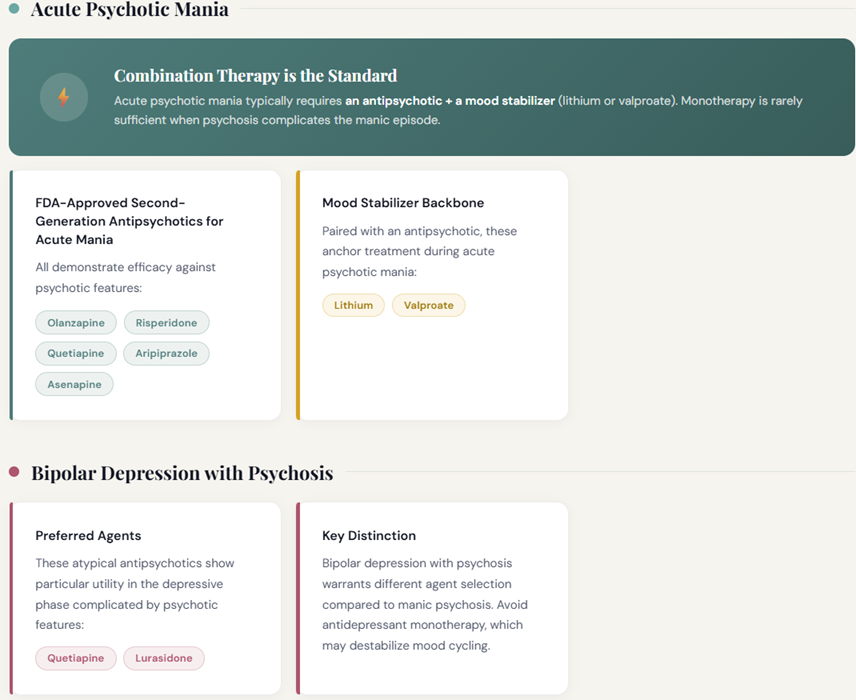
Treatment Considerations in Psychotic Bipolar Disorder
During acute psychotic mania, combination therapy with an antipsychotic and a mood stabilizer (lithium or valproate) is typically required.6
Second-generation antipsychotics including olanzapine, risperidone, quetiapine, aripiprazole, and asenapine are FDA-approved for acute mania with demonstrated efficacy against psychotic features.
Quetiapine and lurasidone appear appropriate for bipolar depression with psychosis.
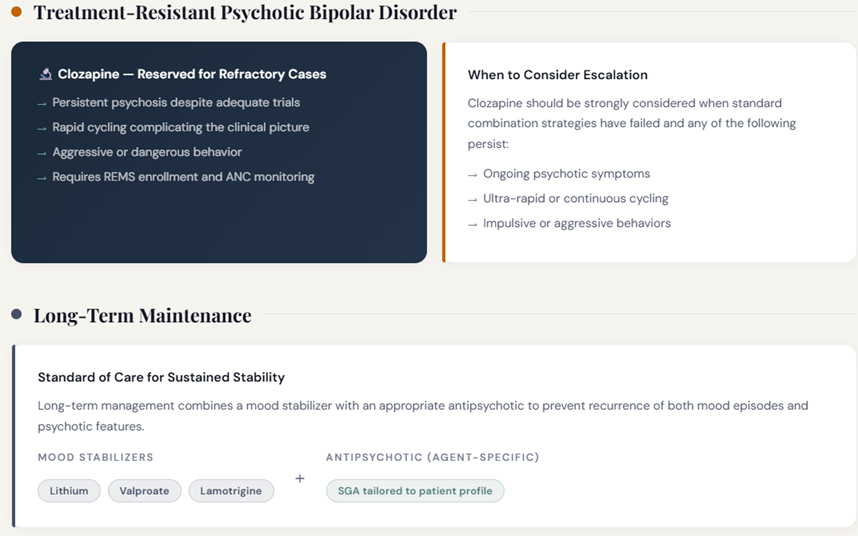
Clozapine should be considered for treatment-resistant psychotic bipolar disorder, particularly where rapid cycling, aggressive behavior, or persistent psychosis complicates the picture.
Long-term maintenance with lithium, valproate, or lamotrigine combined with an appropriate antipsychotic is the standard of care.
 |
 |
|
|
|
|
|
|
|
|
DISCLAIMER
|