|
|
|
|
|
|
|
Medical Pharmacology Chapter 16: Pharmacology of Antipsychotics Drugs
|
|
|
|
|
|
|
Case 2: Chronic Schizophrenia with Tardive Dyskinesia and NonAdherence
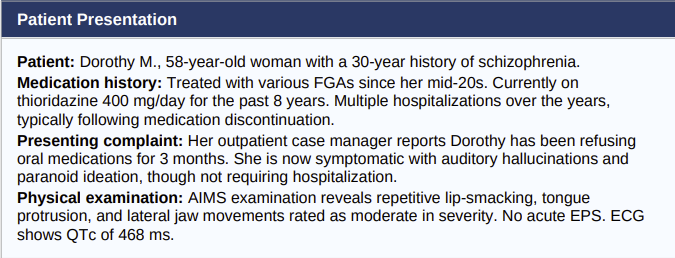
Clinical Course
Dorothy is found to have established tardive dyskinesia by AIMS criteria and a prolonged QTc interval, a combination that makes continued thioridazine both clinically inappropriate and potentially dangerous.
Her non-adherence has resulted in a clinical relapse.
Discussion Questions
1. What concerns does thioridazine pose for this patient, independent of TD?
2. What is the relationship between her current medication regimen and the tardive dyskinesia?
3. What strategies would you employ to address the non-adherence?
4. How would you manage the tardive dyskinesia?
Teaching Points
Thioridazine and QTc
Thioridazine carries a black-box warning for QTc prolongation and torsades de pointes. A QTc >460 ms is already concerning; the drug should be discontinued and replaced with a safer alternative.
Tardive dyskinesia management
TD severity should be assessed using the AIMS at baseline and at regular follow-up intervals.
Per Kane and colleagues' epidemiological work, risk increases substantially with age and duration of high-dose FGA exposure.10
Dose reduction or switching to an SGA (particularly clozapine or quetiapine, which carry lower TD risk) is an important consideration.
VMAT2 inhibitors (valbenazine or deutetrabenazine) are FDA-approved for TD and should be considered for moderate-to-severe cases.
Non-adherence and depot formulation
Dorothy's repeated relapses following oral medication discontinuation make her an ideal candidate for a depot antipsychotic.
Haloperidol decanoate (or an SGA long-acting injectable) administered every 4 weeks would ensure medication delivery and provide regular clinical contact.
This view is consistent with the APA 2021 guideline recommendation for long-acting injectables in patients with uncertain adherence.13,15
Therapeutic alliance
Non-adherence frequently reflects inadequate shared decision making.
A collaborative conversation about Dorothy's concerns regarding side effects, coupled with a concrete plan to address the TD and offer depot therapy as a tool for stability, is more likely to succeed than coercive approaches.
|
|
|
|
|
|
|
|
DISCLAIMER
|